This website uses cookies that help the website function and that help us understand how you interact with it. Please read our privacy policy for more information.
The most recent WHO Classification of Tumours emphasizes the importance of biomarker testing in the diagnosis of brain tumors, yet nearly 70% of patients with brain tumors reported not understanding what biomarker testing is in a recent survey. National Brain Tumor Society launched the MyTumorID campaign this year to educate and empower patients and care partners to make informed decisions about biomarker testing and clinical trials.
Our team recently spoke with Keith Ligon, MD, PhD, who is the Chief of Neuropathology at Brigham and Women’s Hospital and Dana-Farber Cancer Institute (DFCI) and serves as the Director of the Center for Patient Derived Models at DFCI. Read below for part one of this informative interview about pathology and biomarker testing (also known as molecular testing) to help patients and care partners better understand this important issue. Part two of our conversation can be found in a separate blog post.
A: A pathologist is a physician trained to generate a diagnosis for patients. So we’re at that first stage of helping patients to understand which particular disease or tumor type they have. One of the best ways to think about pathologists is that they’re data generators. We try to generate, manage, and communicate to patients and their treatment team information or data on the tumor — what kind it is and what types of approaches might work best against it as far as biomarkers that would help them to navigate that disease.
One thing that’s important for people to understand is that the pathologist writes a report that contains information about what the tumor is, and they layer additional data into that report. Sometimes, that takes a little bit of time. [The pathologist builds into the report] the information that determines all the subsequent treatment and decisions that the treating team is going to make with that patient and what options are available for both standard care and clinical trials. It’s the critical piece that determines the downstream things that happen to a patient and what their prognosis or likelihood of being able to successfully treat it is.
Q: What information is typically included in a pathology report?
A: There are many types of pathology reports. Each test, laboratory test, or examination of tissue that gets done generates another report. So there’s not just one pathology report, although the field is moving to have more of an integrated or comprehensive report that patients can have.
If someone asks, “Well, what did your path report show,” [they are usually referring to the] initial diagnosis. For most patients with a brain tumor, that’s based on the tissue that is removed during surgery. The pathologist examines it as a first step, usually under a microscope, and looks at the cells and what they look like. That initial step, which we call morphology analysis or anatomic pathology analysis, is the general key report that everything else kind of hinges on, and that’s the first time it gets categorized as some type of particular brain tumor in the anatomic pathology report or surgical pathology report.
Pathologists have a lot of experience looking at tumors and have been doing this, as a field, for 100-plus years. We look at the patient’s tissue and write descriptions of it that compare it to and match it with other tumors previously described. It’s categorizing or classifying and distinguishing that tumor from another tumor based on visual images of cells in tissues, through a microscope — not from an MRI scan or CT scan.
That’s the first step to say, “What does this look like? What’s the general category?” And we’re using new tools like artificial intelligence or pattern recognition software to try to assist our human eyes and brain. This type of approach is an exciting area of growth right now due to digital pathology. AI or approaches like it can help us to do more systematic or reliable recognition of tumors and the cells and how they look, and the ability to do it at higher resolution.
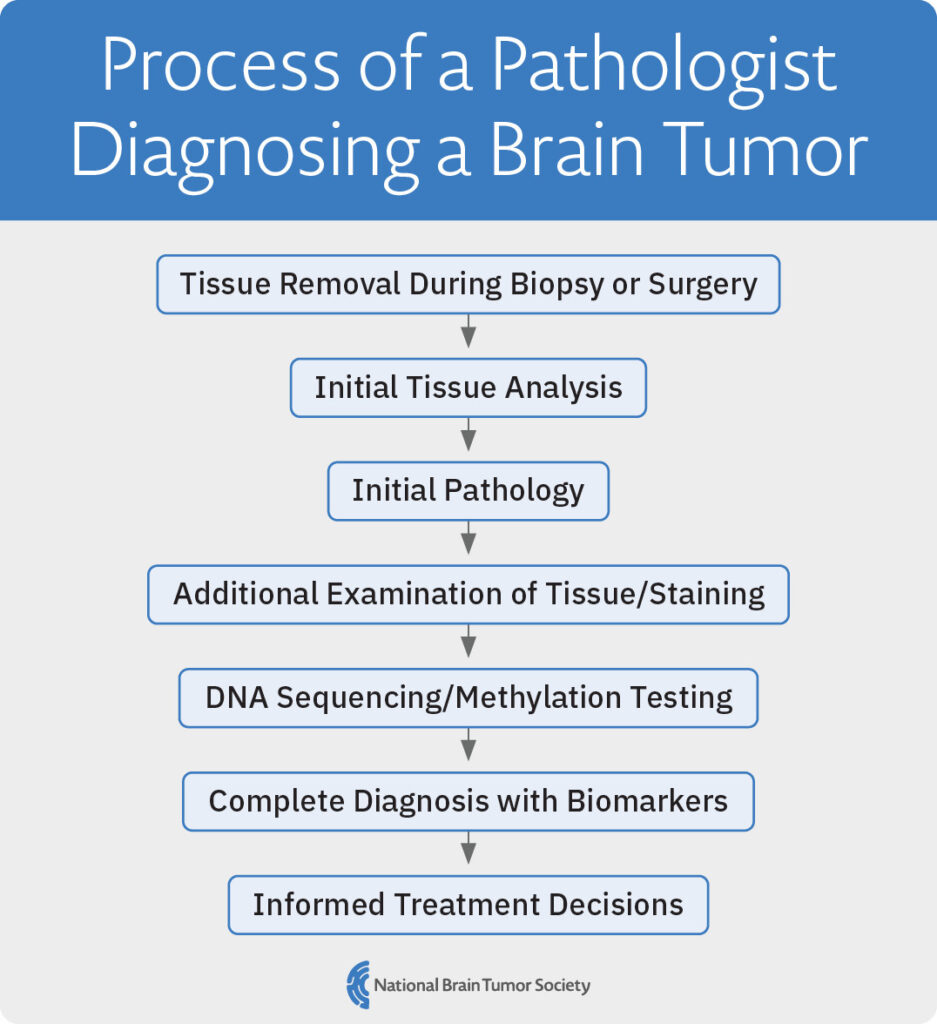
Q: Can you walk us through the process of diagnosing a brain tumor, from getting that initial biopsy from surgery to the final diagnosis?
A: That’s an important one because most patients don’t hear about or have it described to them.
When a surgeon is removing a tumor, they might like to know more information during the surgery. In this instance of an intraoperative diagnosis, pathologists are on call. They obtain the tumor from the surgeon and look quickly to generate that first diagnosis within 20 minutes or less by saying what they see under the microscope. Sometimes, the diagnosis at that early stage is clear. But sometimes it’s not clear and we have to wait for a deeper analysis. This rapid information helps the surgeon to understand whether they are doing the right surgery for that patient.
The pathologist examines all the tissue that comes out to document how much tissue they have and then to preserve it and store it for all kinds of different tests that the patient may need. That’s sometimes difficult because we don’t always know what a patient’s going to need, so we try to store as many things and in as many different ways as possible to anticipate all of the patient’s testing needs. That could mean chemically fixing the tissue so it doesn’t decay. Freezing the tissue is another way of preserving tissue for patients that we do regularly. More recently, in some institutions, we can culture or store the cells alive so that patients can have new and innovative living models of their tumor, including cell lines, xenografts, or other things now used in testing.
The most standard approach used to diagnose tumors is what we call diagnostic histopathology. This approach involves working with the piece of tissue that was chemically fixed and preserved. It’s put into wax and then cut with a machine-mounted razor blade thin enough that we see through the tissue when it’s placed on glass slides, and light is passed through it on a microscope. The tissue is stained with some pink and blue stains called hematoxylin and eosin to see the cells better, and that’s the standard image used for all patients. This visual is the image of tumors we sometimes see in the media or press when talking about cancers.
After the first steps, we do other more complex stains, which will also be described in the patient’s reports. We stain for proteins and those special stains, or immunohistochemical stains, are done to try and really narrow down more precisely what kind of tumor it is, what cells it came from, how fast it’s growing, and what amount of invasion into the brain it might have. All of those are factors that we put in the reports to help estimate how aggressive it might be and what treatments are indicated.
Newer tests and reports that get generated now for patients are things like DNA sequencing analysis of the tumor or methylation profiling analysis. These methods generate a deep and rich pile of data that allows pathologists to compare tumors and, more precisely, predict what decisions you should make with your treatment team and sometimes reveal good news, such as that you’re not going to need further treatment.
Q: How long does it typically take to complete a neuropathology report?
A: Waiting is probably the hardest thing for patients and their pathologist. We understand that, but our job is to get things right. If we get the answer wrong, all your treatment could be wrong. For pathologists or physicians who are trained to be very careful, being careful usually requires more time. We’re intensely focused on faster and faster tests that are also reliable and accurate, and that’s where some of the newer technologies come in.
As a standard example of the time it takes, tumor tissue comes out from the surgery, and there’s a team of expert pathologist assistants and histology professionals who work with the pathologists to help get tissues chemically processed and turned into glass slides. That first step is the one that takes some time. It’s not immediate, so it usually takes at least a day. If you had surgery late in the day, it might take two days because it didn’t come out in time to be processed and preserved long enough to get good results.
Then, we usually look at it under the microscope, and we order more tests to try and determine what the diagnosis would be. This is where there’s a lot of variability. You may hear of one patient who got their diagnosis within a day or two if it’s simple and clear. But if it’s a challenging case and not clear, then we might need to run more advanced tests like staining or sequencing — which can be done in 10 days to a few weeks — to give as accurate a diagnosis as possible that determines what’s going to happen for your care. The timing depends on how hard the diagnosis was or just how many additional tests were needed. Some tumors, like meningioma, don’t require very many tests, while other brain tumors, like glioblastoma, are now often getting many tests performed on them by the pathology team, and it can take a while for them all to come back.
The real truth is that brain tumor diagnoses require a lot of thought, and a great deal of effort is put into it. If your case is unclear, the pathologist may need a lot of consultation — showing it to other pathologists to get their opinions — or additional tests. Usually, by the end of three to four weeks, most of the data has been generated and put into a report. Sometimes you can’t give a good, accurate answer to the patient until you get to the final endpoint of all the tests. The main thing is we try to narrow it down now and issue the information that we can as it’s generated, making sure to be confident of it as we go and then get more specific with more tests.
Occasionally, new data, information, or tests come to light and we do change diagnoses. This is taken very seriously by pathologists and is rare, but if it does happen, it’s important to understand that it doesn’t mean anything was necessarily done wrong. It’s just that more specific information came out that changed our view of the tumor.
Q: How do pathology findings influence treatment decisions for patients with brain tumors?
A: All treatments are designed around a diagnosis. The best way to think about it is as a flow diagram. You would start and say, “Okay, you have a brain tumor.” And then you say, “What are the different kinds?” The different kinds each have different treatment approaches and different effectiveness of those treatments, causing patients to have a different idea about what their prognosis is going to be — both for how long they might be disease-free after treatment and whether they might be cured. Each one of those predictions is based on lots of data around what happened to patients with that tumor in the past.
As an example, if a patient has a low-grade meningioma, WHO grade 1, then there’s a lot of information in the literature and in our decision trees that tells us that type of tumor often is cured or doesn’t come back. Statistically, if you have glioblastoma, which is a high-grade tumor called WHO grade 4, it’s going to be approached with a totally different set of treatments and a different set of decision points that the patient and their treating physician may need to make and decide together. Sometimes, there are different sub-types of tumors, perhaps based on mutations in glioblastoma, where new treatments open up as options through, say, a clinical trial. Or if you had MGMT status, which is an example of a pathology test that gives you an idea of your response to temozolomide. Each of those affects decision-making, so it’s a tiered level of decisions and algorithms for what is appropriate for treating patients as far as our best understanding of how similar patients responded in the past.
Q: What’s the difference between the initial pathology report and when you get the biomarker testing results later?
A: Once you see the tissue and render that first diagnosis [after surgery], there are specific important tests or biomarkers tied to the diagnosis that doctors treating you automatically would want to know. Biomarker is a general term for anything that might be useful data about next decisions, prognosis, or expectations.
The next step is to identify what types of tests or biomarkers are required in order to determine a treatment plan. In some hospitals, a pathology department may have access to more specialized biomarker tests for patients compared to other hospitals that may have more limited testing menus. Some of this can be due to the costs of developing the tests. Some of it can be just the expertise of the pathologists at one place. It can also be that the treating physicians, for instance, at one hospital, differ in opinions of what testing they find important. At most big academic hospitals with medical schools, pathologists do now feel it’s important to have advanced tests such as sequencing for brain tumors. This is, therefore, important for patients to ask about when they are working with their care team to plan treatment.
A: That’s been one of the important and exciting advances in diagnosis over the past years. The WHO represents panels of expert pathologists as well as other physicians taking care of patients with brain tumors coming together and deciding what some of that agreed consensus would be on what biomarkers are important based on research and literature.
It’s important to understand that there is a standardized worldwide consensus that if you have a glioblastoma or a glioma, for instance, it’s then important to test whether you have an IDH mutation or not. That’s from many years of work showing that IDH mutation indicates important biology differences and associated survival differences, with IDH generally being associated with longer survival for patients. It then determines the treatments that you would need to take. Knowing if you have that IDH mutation is probably the most important example of the [value] of sequencing in the field of gliomas right now.
Biomarkers can have different levels of importance. Some are felt to be almost essential for basic understanding of the tumor. There are some that are associated with a difference of someone surviving statistically in large studies — potentially small differences in how the tumor might respond to drugs or to how long the patient might be tumor-free. Some have a big difference in what a patient’s care would be, and others don’t affect care much but are still being understood or studied.
You’ll sometimes see information put into different categories of biomarkers in reports, like for sequencing. Some are important for diagnosis or telling you what the tumor is. Some are important for prognosis and survival. Some are important for what types of drugs might be used and matched to that tumor mutation, so those would be therapeutic-type biomarkers. Each of these is a little different, and we are currently trying to learn how to better label them and help patients, as well as their treating doctors, to understand these results.
Biomarkers are now basically part of the definition of what tumor you have and go beyond just looking at cells, which is a good thing. Now, because we have several biomarker types to help patients, pathologists can deliver more predictable and reliable diagnoses, and be more precise in predictions of how a patient’s tumor is expected to behave.
Q: Does a patient who has experienced a recurrence based on tumor regrowth spotted on a scan need to undergo additional pathology?
A: Usually, the answer is yes. Increasingly, there are options that would be available to you as a patient or decisions that would depend on this re-biopsy to give new information about the tumor. After treatment of your initial tumor, tumors can change and evade treatments. We now know that we can’t assume that the tumor that might be recurring is the same anymore. Some tumors have recurrences that look the same, while in other patients, the tumor changes a lot. Gliomas have the potential to change a lot over time, especially after treatment. So, increasingly, it’s important to biopsy or sample that tissue and get more data and information about the tumor again to help the patient as much as possible. We check to see whether there are any changes and then make a treatment plan based on what’s actually present at that time, as opposed to what might have been there before. It’s not always essential for every patient, for instance, depending on the tumor type, but it is increasingly important, so that’s a great area for patients to reach out and discuss with your pathologist or treating physicians.
Continue reading the conversation with Dr. Ligon in part two.
Learn About NBTS’s MyTumorID Campaign
With the launch of MyTumorID, the National Brain Tumor Society commits to educating patients and their care partners about the value of biomarker testing and clinical trials, empowering patients to ID their tumor, know their options, and make informed decisions about their treatment.
Sign up to receive information about biomarker testing, clinical trials, and more, including updates, educational materials, ways to raise awareness, and future action alerts.