This website uses cookies that help the website function and that help us understand how you interact with it. Please read our privacy policy for more information.
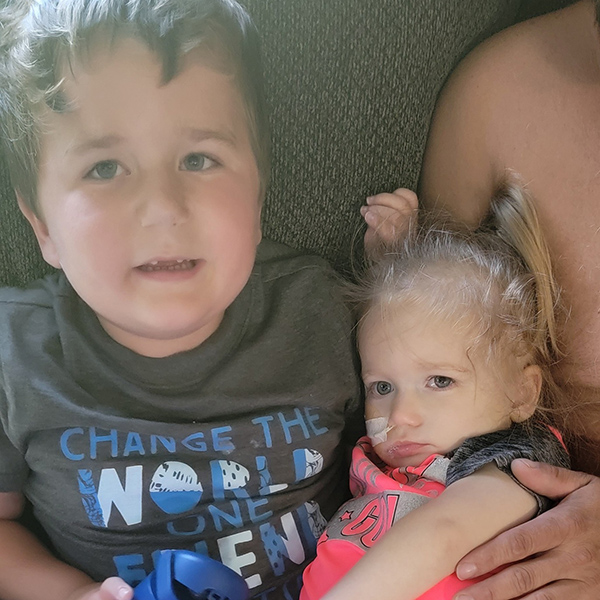
My daughter, Eloise, loves food, puzzles, and the children’s singer Ms. Rachel. She laughs at the littlest things — her big brother Tristan dancing around the living room or her favorite cartoons on TV.
While her brain tumor diagnosis has shaped so much of her young life, it hasn’t dimmed her joy.
The First Signs Something Was Wrong
By the time Eloise was 18 months old, she still wasn’t walking, and an OT evaluation showed left-sided weakness. I then noticed that she started to turn her whole head to look to her right.
In December 2024, things took a frightening turn. Eloise started vomiting and couldn’t keep food down. She was so lethargic that I worried that if she went to sleep, she’d never wake up. We rushed her to the emergency room. After she was given fluids, she perked right up, so they sent us home.
While she was no longer vomiting, Eloise was still experiencing these odd symptoms. My gut told me something was really wrong. Her pediatrician listened to our concerns and sent us straight to neurology. That same day, Eloise had a CT scan.
The Words No Parent Should Hear
The doctor came in and said, “I have some rough news.” I’m thinking that they’re going to tell me she had a stroke or something. Instead, the doctor says, “We found a mass on her brainstem.”
I’ll never forget that moment as long as I live. I remember looking down at Eloise, thinking, “Why is this happening?” We were admitted to the hospital that evening, and she went for an MRI the following day.
While Eloise was getting her MRI, the neurosurgeon talked to us to let us know that the tumor’s location made it inoperable. She told us it was likely a diffuse midline glioma (DMG), which used to be called DIPG. It’s an aggressive, incurable brain cancer, and the doctor explained we would likely have 1-1.5 years with Eloise.
Hearing that news felt like the floor dropped out from under me. The neurosurgeon offered to do a biopsy of the tumor, which would help us figure out what it is, but based on the symptoms and imaging, they believed it was DMG.
We chose to move forward with a biopsy. With our permission, they took a sample for research and a sample to send off for biomarker testing, a way to understand Eloise’s tumor at a molecular level, and to learn exactly what type of tumor it was.
Biomarker Testing Changed Everything
Initial pathology from the biopsy indicated that the tumor was not DMG, but a low-grade tumor, possibly pilocytic astrocytoma. A month later, we received the biomarker testing results, which showed it was grade 1 diffuse astrocytoma with a MYB alteration.
Instead of high-grade brain cancer, it was classified as a low-grade glioma, technically “benign.”
Biomarker testing gave us the confidence to make informed decisions now that we knew the type of tumor she had. It also gave us hope that she has a fighting chance to eventually get better.
That’s why the National Brain Tumor Society launched the MyTumorID campaign to help educate patients, caregivers, and families about the importance of biomarker testing to receive an accurate diagnosis and make informed decisions about treatment options.
He knew something was wrong. When my mom asked how he was doing, he told her, “My mom and dad are in the hospital with my baby sister. When are they coming back in 18 days?”
When we picked him up the next day, I sat him down and said: “Eloise has something called a brain tumor. It makes it hard for her to walk. She has to get special medicine, and Mommy and Daddy are hoping it will help her get better, but there’s a chance she might not.”
He looked at me with wide eyes and asked, “Mommy, why are you crying?”
I’ve tried to be honest with Tristan without overwhelming him. For a while, he thought everyone who went to the hospital must have a brain tumor. We had to gently help him understand that it wasn’t true.
When we later got the news that Eloise’s tumor wasn’t DMG, I told him, “Things are looking a little better. Eloise is going to get special medicine, and eventually it sounds like she’ll be able to walk and do things, but it’s going to take time.”
Being honest with him has always mattered to me.
Balancing Work and Caregiving
I’m also a Title I math teacher in a small school district with about 350 kids. From the beginning, my principal and superintendent told me to do whatever I needed to take care of Eloise.
I’ll never forget when the superintendent called me and said, “Here’s what you’re going to do. You’re going to use your days, file your FMLA paperwork, and then take a leave of absence. Don’t worry, we’ll approve it. Take the time you need.”
That kind of support meant everything. It allowed me to focus on Eloise without worrying about losing my job. When her doctors later encouraged us to let her go back to daycare once a week, they also told me I could think about returning to work part-time.
Even my husband’s employer has been supportive, paying him for the days he missed for Eloise’s appointments. It’s one of the biggest blessings in this whole nightmare, knowing our workplaces have wrapped around us so we can focus on our daughter.
From Chemotherapy to Proton Radiation
Because Eloise did not have any mutations that would open the door to targeted therapies, she began chemotherapy. Her tumor didn’t shrink, but it stopped growing for a time, and that gave us hope.
Unfortunately, the tumor began to grow again, and we have now moved on to proton beam radiation therapy. We arrive at the Proton Therapy Center every morning at 7 a.m., five days a week, for six weeks straight. She goes under anesthesia so the doctors can safely target her tumor, and we’re usually done by 8:30 a.m.
I am hopeful this works. But if it doesn’t, I’m not giving up. I was ready to go to the ends of the Earth when they thought she had DIPG, and I’m still willing to go anywhere and try anything that might help her.
Her doctor told us they wouldn’t try proton therapy if they didn’t think it had a chance to help. It may stabilize Eloise’s tumor. It may shrink it, or it may not work at all. But this treatment gives us the best chance right now.
Moving Forward
Eloise has already faced more in two years than most people face in a lifetime. She’s been through chemo and now radiation. She has physical challenges that make everyday tasks difficult. If there were a way I could switch places with Eloise, I would in a heartbeat.
I like to explain that cognitively speaking, she’s two years old, but she’s stuck in an 8-month-old body because it’s hard for her to get around. She loves to lie down and play, and we’re trying to work on her sitting up.
That’s why I created the “Eloise Strong” ribbon — a blend of yellow for childhood cancer awareness and gray for brain tumor awareness. Eloise’s fight deserves both. She deserves recognition in both September (Childhood Cancer Awareness Month) and May (Brain Tumor Awareness Month).
This isn’t just about Eloise. It’s about every child navigating pediatric brain tumors and cancer. These kids endure treatments most adults couldn’t handle. They show courage every single day. They are heroes, whether they are still fighting, in remission, or have earned their eternal rest.
We need more awareness, more research, and leaders who will prioritize pediatric cancer and brain tumor research.
We don’t know what the future holds. But all we can do is take everything one day at a time, just like we have since December 7, 2024, when she was first diagnosed with a brain tumor. We have to have faith, a positive mindset, and hope, but also have to be pragmatic, practical, and realistic.
Childhood Cancer Awareness Month
While brain and other CNS tumors are the most common form of solid cancer in children in the U.S., treatment options for children with brain tumors are far too limited. For adolescents and children with a pediatric brain tumor diagnosis, it’s time for a better chance.
Childhood Cancer Awareness Month (CCAM) is a time to recognize, advocate for, and honor children who have been affected by cancer and the families that care for them. This September, the National Brain Tumor Society invites you to make a gift and help NBTS continue to accelerate pediatric brain tumor research, advocate for change, and provide connection and navigation to children and their families.