More than 17,000 Americans will be diagnosed with a pituitary tumor each year, accounting for 17.4% of all brain and CNS tumors. In fact, pituitary tumors are the second-most common benign brain tumor, behind only meningiomas.
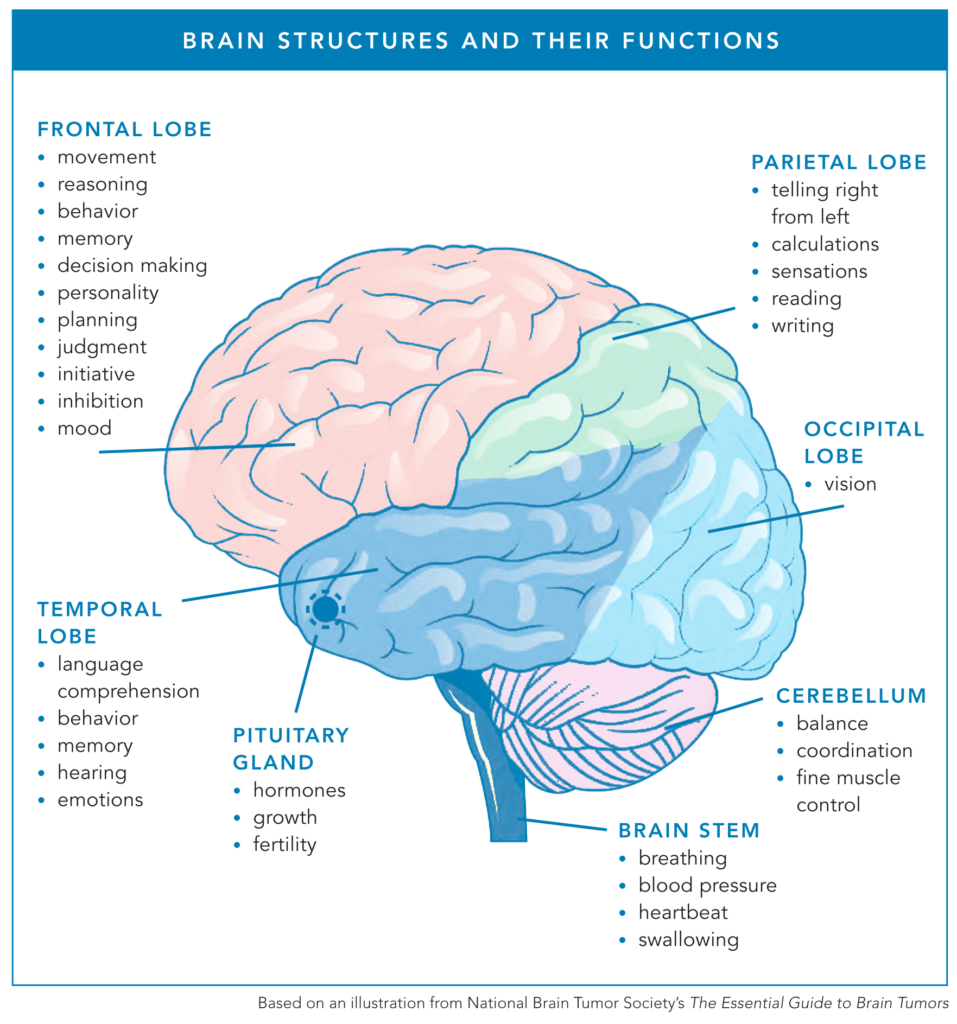
The pituitary gland is a small, pea-sized gland located at the base of the brain, behind the nose, that produces and releases hormones. Often called the “master gland,” the pituitary is attached to and interacts with the hypothalamus to regulate essential body functions, such as growth, metabolism, and fertility.
Just as a thermostat turns off the furnace once the room reaches a set temperature, the pituitary gland stops producing a hormone once it senses that there is enough in the bloodstream. For example, if someone’s thyroid hormones (T3 and T4) are low, the pituitary gland will “turn up the heat” by releasing more thyroid-stimulating hormone (TSH) to increase the body’s thyroid hormone levels. Once thyroid levels return to normal, the pituitary gland “turns off” and stops secreting TSH.
Pituitary tumors, also called pituitary adenomas or pituitary neuroendocrine tumors (PitNETs), occur when DNA mutations in pituitary gland cells lead to uncontrolled cell growth.
Let’s talk about what makes pituitary tumors different from other brain tumors and learn more about the experiences people living with this tumor type may face.
Common Symptoms
Most pituitary tumors do not cause symptoms, and these tumors often go undiagnosed. Mayo Clinic reports that about 1 in 10 people have small pituitary growths, which are only found during routine imaging, bloodwork, or an autopsy.
However, when a pituitary tumor grows large enough or disrupts the pituitary gland’s function (by producing too much or too little of a hormone), it can cause symptoms such as headaches or vision changes.
“My tumor was quite large (23 millimeters), so it was pressing on my optic nerve,” Ashley D-L. said. “My vision was rapidly declining. It went from a blind spot to almost complete blindness in my right eye. No one could tell me if I could get my vision back. I had surgery, and I could see perfectly when I woke up.”
While these tumors are often benign, they can impact normal pituitary function by causing one or more essential hormones to be produced too little (known as hypopituitarism) or too much (known as hyperpituitarism).
Signs and symptoms for pituitary tumors impacting hormone production vary based on which hormones are impacted, but can include:
- Fatigue
- Weight loss or weight gain
- Dizziness
- Muscle weakness
- High or low blood pressure
- Irregular or absent periods
- Galactorrhea (milk discharge in people who are not pregnant or breastfeeding)
- Sexual dysfunction
- Infertility
Typically, doctors perform brain imaging and blood tests to measure hormone levels to confirm the diagnosis. Vision tests may also be needed.
One of the biggest challenges for people with pituitary tumors is that their symptoms can easily mimic those of other illnesses or diseases, delaying the discovery of the pituitary tumor.
Lived Experiences
Brain tumor community members generously shared the signs and symptoms they experienced before they were diagnosed with a pituitary tumor.
“The symptoms that I had were also like mid-life, perimenopausal, stressed-out mom symptoms. I could just tell that something wasn’t right, but I thought it was an autoimmune disease or something like that. My doctor said my bloodwork came back normal.
So I did one of those at-home thyroid panel blood tests because my doctor would only test my T3 and T4. I had done so much research on my own that I realized there were other tests we should include. The results were pretty bizarre. When I researched what those low results could mean, I read that it usually means a pituitary tumor.
I figured that wasn’t likely, so I just dealt with symptoms for two years. During that time, my anxiety felt uncontrollable. I was gaining weight and couldn’t lose weight. I worked out fairly regularly, and I ate pretty clean, but it didn’t matter. All of a sudden, my skin, mouth, and nose were so dry. It felt like a full-time job keeping all these things hydrated. I slept all the time.
In March 2022, it was as if a switch had flipped. I went from occasional migraines to having two to three migraines a week. My doctor said it was hormones and to wait it out, despite my seeing her every six weeks about my symptoms. When my doctor left the practice, I saw a new doctor, who immediately referred me to a specialist.
Later that year, I was on a girls’ trip and realized I had a blind spot in my eye. An ophthalmologist sent me for an MRI scan, which showed a tumor.
Before surgery, my testosterone was undetectable, my cortisol was a tad high, and my prolactin was high because of the stress, but not as high as a prolactinoma. After surgery, I had no more headaches. About 10 months post-op, my thyroid-related issues have calmed way down.” — Ashley D-L.
“To be honest, I don’t think I personally remember a lot of my 20s. What I really remember is me sleeping a lot and my social life revolving around napping. I used to be like a three-sport athlete who played year-round and was always on the go. And then my energy levels just plummeted in my early 20s. I was tested for narcolepsy and PCOS. Nobody could really find what was wrong with me.
When I turned 30, I started working with a nutritionist and things like that, and I slowly started getting migraines, which I’d never really dealt with before, and they really affected my right eye. It got to the point where I was getting three a month, and they were debilitating, lasting a week. I don’t know how I still had a job at that point. My boss pulled me aside to talk about it, and that’s when I went to urgent care and eventually got a CT scan of my head. They discovered the mass at that time, so I went to the ER.
There, the endocrinologist explained a lot to me, including what the pituitary should do and how mine was functioning differently. To be honest, I don’t remember the full details. I just remember her saying, ‘This is what your pituitary should look like, and this is what your pituitary looks like. She then explained how surgery could be effective.
The only advice I can give to people is to advocate for themselves. If you feel like something is wrong, don’t stop until you feel like you really get answers. I had to switch doctors a couple of times and get second opinions.” — Abby P.
“I was skinny my entire life. I was 100 pounds when I graduated high school, and then all of a sudden, I gained all this weight, and people thought it was from just me overeating and not taking care of myself. There was something underlying going on, and people don’t seem to understand that.
I had gained about 50 pounds, and my OB/GYN thought it was a little suspicious. She did the bloodwork, which showed that I had really high prolactin levels. She had me get an MRI to be safe. As I was cutting my birthday cake on my 28th birthday, the notification came over the portal that I had a tumor.
Over the following weeks, I had a lot of bloodwork, I had a lot of doctor’s appointments, and they started me on cabergoline [a medicine used to treat high prolactin levels] immediately. At first, my OB/GYN did all the care for it. After six months, my prolactin levels weren’t improving, so then I started seeing an endocrinologist. Thankfully, [my tumor] is so small that they’re not going to be doing surgery on me.” — Alexa Y.
“I started to gain weight out of nowhere. I didn’t really know what was going on, but I knew something was wrong. I went to multiple physicians who regrettably didn’t treat me with tons of respect. I had an MRI that revealed a tiny tumor, but I was told it was nothing.
My dear friend, who was a testicular cancer survivor, said to me, ‘You’re just not yourself. You need to be your own advocate.’
I took his advice and self-referred myself to the Mayo Clinic. The endocrinologist I met with diagnosed me with my first pituitary tumor that day.
My second tumor (corticotroph adenoma) was found on the other side, and they didn’t see it when they were in there the first time. Regrettably, the second one came back because they couldn’t get all the margins, so that’s when I had Gamma Knife [a form of surgery using targeted radiation].
I credit Mayo Clinic for saving my life and the National Brain Tumor Society for empowering it.” — Amanda M-L.
“The only reason I know that I had a prolactinoma was because I had a blinding migraine after brunch one day. I ended up having to take the whole work week off. I did a telehealth appointment, and she said I needed to get an MRI. By the time I was able to get an MRI, it had subsided a little bit with migraine-focused medicine.
The radiologist said it was a macroadenoma, which is a tumor greater than 1 cm in diameter at diagnosis. Once we got past the initial shock of it and learned that the pituitary tumor was called prolactinoma, it was more game plan mode. I need an endocrinologist. I need a neurologist. I don’t need surgery. I’ve been on cabergoline, and it seems like I’m responding well.
Working with the endocrinologist ended up being the best option.
We want to get pregnant, but with the prolactinoma, it would be hard to get pregnant already, and then she doesn’t want me to get pregnant while on the cabergoline. There’s at least a year before we can even think about trying, which sucks.” — Amber T.
“Back in 2017, I had constant headaches, and my ex was taking me to the ER a lot. I also had lactation out of my breast. One nurse finally asked me, ‘When was my last menstrual cycle?’ And I told her, ‘Two years ago.’ She had me do a CT and then an MRI, which discovered the mass.
I had surgery, and then it returned in a year and a half. My headaches were too bad. I lost hope and drowned myself in alcohol to numb the pain.
I later met my now husband, and then I decided to try again. I stopped drinking and sought medical care for my tumor. They removed the tumor, but there’s underlying effects. I’ve had a headache every day for 10 years.
I can hold a normal conversation. I can go out in public, and I am smiling. But all of these symptoms – they are hidden. I can mask my pain very well. People don’t know I just had an emergency room visit because I passed out in the Walmart parking lot.” — Dominique G.
“During my pregnancy, I gained almost 100 pounds. I wasn’t really the kind of pregnant woman who had cravings and was eating all this food. When I had my daughter, I was having a really hard time losing my pregnancy weight. We’ve always been very active — exercising, hiking, running, skiing — so it was very strange to me what was going on in my body.
I saw an endocrinologist at my husband’s recommendation, and she did a really extensive panel on me. First, she found my thyroid was off. She decided to test for elevated insulin-like growth factor-1 (IGF-1), which isn’t a common test, and it was totally off the charts.
A neuro-endocrinologist sent me for an MRI, which found a pituitary tumor. My high IGF-1 indicated acromegaly [a rare condition caused by the presence of excessive growth hormone], and I went into remission from acromegaly after my surgery.
I took two months off work due to extreme fatigue and some vision changes initially. The pain was not as bad as my two C-sections, but the fatigue was really unexpected. I felt the fatigue lifting a bit about six to eight months after surgery.” — Ivy A-L.
“Back in 2018, the only symptom I had was a headache. It would only happen at night when I’d be dead asleep. It was behind my right eye. It felt like someone was jabbing a knife in the backside of my eye and just twisting it. It wouldn’t happen regularly, but toward the end, it got to the point where it was every night.
The day I was diagnosed at the age of 47, my wife had found me unresponsive, and they rushed me to the hospital.
Surgery removed 95% of the tumor, so there’s still 5% of it remaining. Knowing that they’re going to watch it makes me feel a little bit better. After I made it through surgery, my personality changed back to normal, and I finally realized that I was given a second chance in life.” — Mark L.
Types of Pituitary Tumors
While pituitary tumors are not graded like many other brain tumors, they can fall into different categories.
Nonfunctioning Pituitary Tumors
Nonfunctioning tumors do not produce hormones, making up about one-third of all pituitary tumors.
Most nonfunctioning pituitary tumors are macroadenomas, tumors that are greater than 1 cm in diameter at diagnosis. These tumors are often diagnosed later when the tumor becomes large enough to cause symptoms.
A very rare subset of nonfunctioning tumors, called pituitary carcinomas or metastatic PitNETs, can be cancerous. These malignant tumors make up about 0.1-0.5% of all pituitary tumors and may be treated with chemotherapy.
Functioning Pituitary Tumors
Functioning tumors do produce hormones, and the excess hormones cause symptoms. As Yale Medicine explains it, “The individual cells that make up the pituitary specialize in producing different hormones. When a tumor forms from one of these cells, it also produces the hormone made by that cell.”
These tumors are typically, but not always, microadenomas because they’re often less than 1 cm. Although smaller, they are usually diagnosed earlier due to symptoms caused by the elevated hormone levels. In fact, the American Association of Neurological Surgeons (AANS) reports that “approximately 50% of pituitary adenomas are diagnosed when they are smaller than 5 millimeters in size.”
The pituitary gland produces and releases six main hormones:
- Adrenocorticotropic hormone (ACTH)
- Follicle-stimulating hormone (FSH)
- Growth hormone (GH)
- Luteinizing hormone (LH)
- Prolactin
- Thyroid-stimulating hormone (TSH)
The pituitary also secretes two other hormones made by the hypothalamus:
- Antidiuretic hormone (ADH or vasopressin)
- Oxytocin
The most common functioning pituitary tumors arise from abnormal growth in cells that specialize in one of the above hormones.
Prolactin-producing tumors called prolactinomas are the most common hormone-secreting pituitary tumors, accounting for 40-60% of adenomas, according to UCSF.
This type of pituitary tumor creates too much prolactin (hyperprolactinemia), which impacts men and women differently.
In women, it can cause irregular or absent periods, breast enlargement, milk discharge, low sex drive, vaginal dryness, osteoporosis, and sometimes infertility.
“I was having irregular periods and really odd period symptoms,” Amber said. “My breasts were very painful a lot of the time. They sometimes had milk come out of them. The first time that happened, I almost had a panic attack seeing milk coming out of my breast when I wasn’t pregnant or breastfeeding at all.”
In men, an overproduction of prolactin can suppress FSH and LH, leading to low testosterone that may decrease libido, reduce body and facial hair, and cause erectile dysfunction. Like women, it can cause breast enlargement and milk discharge in some cases.
People with prolactinomas may also experience weight gain.
Somatotroph adenomas are pituitary tumors that produce too much growth hormone (somatotropin). This type of tumor is found in approximately 20% of all pituitary tumors, according to the International Journal of Endocrine Oncology.
Gigantism
These adenomas can cause gigantism in kids due to the abnormal, rapid growth before their growth plates close.
Signs and symptoms of gigantism may include:
- Larger in size than their peers
- Changes in facial features
- Delayed puberty
- Irregular periods (females)
- Excessive sweating
- Teeth gaps
- Enlarged organs
Acromegaly
Acromegaly is a rare condition caused by the presence of excessive growth hormone in patients after their growth plates have closed. According to the International Journal of Endocrine Oncology, more than 95% of cases of acromegaly are due to somatotroph adenomas.
“When I was diagnosed, my growth hormone levels were in the thousands, when someone my age should be in the two to three hundred range,” Abby said.
Signs and symptoms of acromegaly can include:
- Changes in facial features
- A deeper voice
- Course body hair
- Swelling of hands and feet
- Sleep apnea
- Carpal tunnel syndrome
- Fatigue
- Excessive sweating
Amanda said, “At my initial appointment, the endocrinologist asked me to show him my driver’s license, which seemed odd. He said, ‘You don’t look like this anymore. Your face has started to widen.’ He diagnosed me that day with acromegaly due to my pituitary tumor.”
Corticotroph adenomas are adrenal corticotropic hormone (ACTH)-producing pituitary tumors responsible for Cushing’s disease, a condition caused by too much cortisol in the body. Cortisol is the stress hormone produced by the adrenal gland. In addition to handling the body’s fight-or-flight response, cortisol also helps regulate metabolism, blood pressure, and blood sugar levels, following the wake/sleep cycle.
Corticotroph adenomas release excess ACTH, which tells the adrenal glands to keep making cortisol.
Symptoms of too much cortisol may include:
- Unexplained weight gain (particularly in the neck and stomach)
- Diabetes
- High blood pressure
- Depression
- Irregular or absent periods (females)
- Osteoporosis
- Purple stretch marks
- Muscle weakness
- Easy bruising
Accounting for less than 1% of all pituitary tumors, thyrotropinomas are pituitary tumors that produce thyroid-stimulating hormone (TSH). Due to the excess TSH caused by the tumor, the thyroid gland releases too much thyroid hormones (T3 and T4), causing a condition called hyperthyroidism.
Signs and symptoms from thyrotropinomas can include:
- Racing heart
- Anxiety
- Difficulty sleeping
- Sweating
- Unexplained weight loss
- Tremors
- Frequent bowel movements
Gonadotroph adenomas are rare pituitary tumors that produce excess gonadotropins — follicle-stimulating hormone (FSH) and luteinizing hormone (LH).
FSH is a hormone made by the pituitary that, in women, tells the ovaries to produce follicles and grow eggs, and in men, tells the testes to make sperm.
LH is a hormone made by the pituitary gland that triggers the reproductive system, specifically causing ovulation (release of eggs) in women and stimulating the production of testosterone in men. By managing these processes, it plays a vital role in ensuring fertility and maintaining the body’s balance of sex hormones.
Signs and symptoms will vary by sex and may include:
- Infertility
- Irregular periods (females)
- Ovarian hyperstimulation syndrome, causing enlarged ovaries and ovarian cysts (females)
- Enlarged testicles (males)
- Deeper voice (males)
- Rapid facial hair growth (males)
- Early puberty (children)
Headaches and visual changes can occur when the tumor becomes too large.
Treatment Options
Not all pituitary tumors require treatment. Incidental findings, for example, where the patient is not experiencing any symptoms, may warrant a “watch and wait” approach. Monitoring, which includes routine imaging and bloodwork to check hormone levels, may be all that’s needed at the time.
Surgery
Surgery is needed for pituitary tumors when they become too large, cause vision changes, or produce excess hormones that cannot be managed by medication. Many small nonfunctioning pituitary tumors and prolactinomas do not require surgery.
When surgery is necessary, neurosurgeons typically perform a transsphenoidal surgery (removal through the nose) rather than a traditional craniotomy (removal through the skull) to remove the pituitary tumor.
“There are very rare cases that the tumor really goes beyond the area of the pituitary or becomes so large that the tumor cannot be safely removed through the nose, and then we have to use a transcranial approach,” said neurosurgeon Aaron Cohen-Gadol, MD.
Transsphenoidal surgery is a specialized surgical approach to access the pituitary gland and nearby structures through the nasal cavity and sphenoid sinus using a thin tube with a camera (endoscope).
“For tumors around the pituitary gland, the best approach is through the nose using an endoscope,” Dr. Cohen-Gadol said. “It’s extremely effective, minimally invasive, and much easier to recover from than going through the skull.”
Radiation
Radiation therapy may be recommended for the treatment of pituitary tumors in a few instances:
- When the pituitary tumor cannot be removed through surgery
- Either to prevent tumor regrowth or to address tumor regrowth
- When medications and/or surgery cannot address the signs and symptoms caused by the excess hormone levels
Radiation therapy for pituitary tumors includes traditional X-rays, precise proton therapy that stops directly at the target, and non-invasive stereotactic radiosurgery. While the first two are often delivered in small doses over four to six weeks, radiosurgery acts like a scalpel, destroying the tumor in one or a few highly targeted sessions.
“I’ve been on medications since six months after my surgery,” Abby said. “I’m actually going to be meeting with a radiologist to discuss radiation because my medications haven’t worked.”
Medications
For functioning pituitary tumors, medications can be used as part of treatment to either stop the tumor from producing excess hormones or to block those hormones from affecting the rest of the body.
Prolactinomas
In some cases, like with prolactinomas, medication is so effective at shrinking the tumor that surgery may not even be necessary.
According to AANS, “With medical management, about 80% of patients have prolactin levels restored to normal through dopamine agonist therapy.”
Dopamine agonists (cabergoline or bromocriptine) mimic a natural brain chemical that tells the pituitary to stop making prolactin. These medications are highly effective at both lowering hormone levels and shrinking the tumor, so medication is usually the first course of treatment.
“At the beginning of taking cabergoline, I had a lot of side effects, and my life was basically put on hold because of it,” Alexa said. “But the longer I’ve been on it, I’ve been on it since 2022 now, I’ve gotten used to it. I do have nausea, but I take Zofran for it, and I’ve found ways to combat it. I noticed that if you take the medication at night, you experience fewer side effects.”
Somatotroph Adenomas
Functioning pituitary tumors that secrete too much ACTH (somatotroph adenomas) cause excess growth hormone. While surgery is typically the initial treatment, medications may be used if surgery is not an option or if surgery cannot remove the entire tumor.
According to the Mayo Clinic, somatostatin analogs (octreotide, lanreotide, or paltusotine) act as a brake on the pituitary gland, blocking the production of growth hormone. Another medication option for some patients is a hormone blocker called pegvisomant that can act like a shield, blocking the excess growth hormone from causing tissue growth and heart issues.
Long-Term Symptom Management
The pituitary’s role as the “master gland” in the body means that recovery from a pituitary tumor often involves long-term management of a variety of symptoms.
“My pituitary tumor presented more challenges than I thought it would,” Abby said. “My team referred to the pituitary tumor as the gland of well-being. Your pituitary does a lot more for you than you might realize. My thyroid was affected. Even though I’m fairly active, I struggle to lose weight. I’m now a type two diabetic.”
Patients usually work with an endocrinologist to monitor hormone levels and manage symptoms.
“I know it affected my testosterone,” Mark said. “It also affected my sex drive and my thyroid. I’m on daily thyroid medication and testosterone gel. Finally, within the last six months, the numbers have started to come back up.”
For those living with a benign brain tumor like a pituitary tumor, benign does not necessarily mean harmless or easy. That’s why the phrase, “benign is not fine,” tends to resonate with many people living with pituitary tumors.
“We were hopeful that my thyroid issues would resolve, but they didn’t,” Ivy said. “I still take thyroid medication every day. I do get headaches from time to time. I still have some vision changes. It’s not significant, but when I’m at a computer, the words are kind of moving around, so that’s hard.”