This website uses cookies that help the website function and that help us understand how you interact with it. Please read our privacy policy for more information.
It usually starts with something small. Ringing in the ear or vertigo that won’t go away. Extra clumsiness at work. Struggling to hear others in a restaurant. People explain these symptoms away as sinus infections or a part of aging, but for an estimated 6,035 Americans every year, they are the first signs of an acoustic neuroma.
About 50% of these benign tumors, also called vestibular schwannomas, occur in people aged 40 to 64, according to CBTRUS.
“This is a benign tumor, but because of where it arises, it’s particularly valuable real estate,” said neurosurgeon Christopher Jackson, MD, Director of the Acoustic Neuroma Center at Johns Hopkins. “It’s located in the cerebellopontine angle — the tight space between the pons and the cerebellum — which carries nine of our 12 cranial nerves. Because these nerves control critical functions from swallowing to hearing and balance, a tumor doesn’t have to be very big to cause serious problems. It’s a high-value neighborhood, which is why we take it so seriously.”
Let’s talk about what makes acoustic neuromas different from other brain tumors and learn about the unique experiences and challenges that come with a diagnosis. For the purposes of this blog, we will use acoustic neuroma and vestibular schwannoma interchangeably, while recognizing they refer to the same diagnosis.
Patients most often experience single-sided hearing loss and persistent ringing (tinnitus) in one ear. Johns Hopkins reports that 90% of patients experience hearing loss in one ear, which typically changes gradually. About 5% of people with acoustic neuromas experience sudden hearing loss.
“The most common symptom is hearing loss, which is how it got the name acoustic neuroma to begin with,” Dr. Jackson said. “Ironically, there’s neither a neuroma, nor does it come from the acoustic nerve, but [they called it that] because people presented with hearing loss and acoustic neuroma had just had a better ring to it than vestibular schwannoma.”
Because the tumor arises from the insulating cells (Schwann cells) of the vestibulocochlear nerve, which plays a role in balance, nearly half of patients with acoustic neuroma experience dizziness, vertigo, and imbalance, according to Johns Hopkins.
Other less common vestibular schwannoma symptoms include:
Ear fullness
Facial weakness or twitching
Facial pain or numbness
Swallowing problems
Hydrocephalus (fluid buildup in the brain)
Neurofibromatosis Type 2
About 5% of all acoustic neuromas are due to a rare genetic disorder called neurofibromatosis type 2 (NF2), which can cause symptoms in both ears.
Lived Experiences
Brain tumor community members generously shared the signs and symptoms they experienced before they were diagnosed with a vestibular schwannoma.
“In January 2025, I woke in the middle of the night feeling like my world was spinning — vertigo, nausea, vomiting, and a clogged ear. Panic-stricken, I woke my husband and literally blurted out, ‘What if I have a brain tumor?’ We assumed it was the onset of a stomach bug and eventually went back to sleep, completely unaware of the reality we were about to face.
The next day, my condition worsened. I couldn’t keep anything down, and my balance deteriorated to the point I needed help walking even a few steps. Dehydration ultimately sent us to urgent care, where IV fluids barely made a dent in my symptoms. The doctor checked my ear canal, found nothing abnormal, and suggested it could be an inner ear problem.
A visit to the ENT and a failed hearing test later, I was first diagnosed with sudden sensorineural hearing loss. I immediately began aggressive steroid treatments — oral and injectable — in a desperate attempt to restore hearing. But after four weeks, there was no improvement. I was still profoundly deaf in my left ear.
As standard protocol, an MRI was scheduled. I already knew something bigger was going on. I could feel it.
Approximately 1 in 100,000 Americans develop an acoustic neuroma each year, according to the NIH. I knew I was that one, and the scan confirmed it: there was a tumor pressing against my vestibulocochlear nerve, which is responsible for balance and hearing. Despite its small size and noncancerous nature, it had already taken my hearing for good.” — Allison L.
“Last April, my daughter brought home this terrible cold, and we all got the cold. And then I noticed that my hearing just wasn’t the same in my right ear. I started getting tinnitus and noticed that my hearing wasn’t bouncing back. While running, I noticed the lip on my right side and tongue were going numb. I surfed and started noticing my balance just wasn’t as good as it used to be.
I watched it for about a month or two and talked to a couple of ENT friends. I had bladder cancer five years ago, so when the symptoms kept persisting, I knew this didn’t add up. I insisted on getting an MRI. I got diagnosed with a 2.7-cm acoustic neuroma.” — Christopher S.
“At first, I thought my symptoms were just a cold or a sinus infection. I felt like a hypochondriac because my dad had recently lost his hearing in one ear, and I thought I was being ridiculous. Looking back, I had occasional dizzy bouts and light balance issues — like struggling to stand on one foot in an exercise class — but I could explain it away.
I noticed my hearing loss when I realized I couldn’t understand people on the phone or hear a whisper in a movie. One night, I lay my ‘good ear’ down on a pillow, and when my husband spoke to me, I realized I couldn’t understand a single word he said. I’ve heard from other people and from doctors that sometimes it’s like the nerve does well until it doesn’t. I felt like I could hear until the sudden moment I felt like I couldn’t.
When I finally went in for an audiogram, the results showed I already had severe hearing loss in my left ear. My doctor sent me to a specialist for an auditory brainstem response test, but the results were inconclusive. He ordered an MRI just to check for a rare brain tumor, though he told me I almost certainly didn’t have it because he had only seen six in his entire career. The very next day after the scan, I got the phone call: ‘You have a brain tumor. It’s an acoustic neuroma.’” — Emily T.
“It was honestly a really slow discovery. I noticed a lot of things over the course of a couple of months, so I was writing them down on my phone. One thing I noticed was that my balance wasn’t quite right. My balance would seem fine at work until I was walking side-by-side with somebody, and I would stumble into them, or take an extra wide turn walking around a corner.
I was still able to listen to music, but it just sounded very flat and muffled in my one ear. It just didn’t sound as clear.
One night, I was trying to type on my computer and kept hitting the wrong keys. I tried using my piano keyboard, and I was playing my song really weirdly. I tried touching my finger and thumb, and then my middle finger and thumb — doing that as fast as I could. I noticed my left hand would sometimes miss my own thumb, even at a really slow speed. That was pretty concerning for me because I figured only something with my brain could cause me to miss my own thumb.
Along with that, the left side of my face was starting to become tingly. I was noticing a lot of the symptoms that I was having had to do with the left side of my body. I also had nystagmus (involuntary, rapid movement) in my left eye, so I’m over here just trying to figure out these symptoms, while still trying to go to work and do my normal everyday activities.
At one point, I finally told my parents, and they thought I was having a stroke. They urged me to go to the ER and get it checked. I left work early that day, and I went to the ER. The nurses and everyone were freaked out that I waited so long when I was telling them my symptoms, and they ordered a CT scan. That’s when they sat me in a room and told me that they found something growing in my brain that was the size of a strawberry.
I was transferred to UCSF, where they told me it was an acoustic neuroma.” — Jonathan J.
“I was majoring in elementary education and special education. For my major, I needed a hearing screening done, so I did it, and they said I had mild hearing loss. I was told to go for further testing with an audiologist. They asked me to come back to do a balance test, which I failed. They sent me for a CT scan, which is when I found out. The acoustic neuroma was just under four centimeters.” — Kat C.
“When you get stationed at any new Air Force Base, they do an intake. So you have to see mental health, public health, dental, family practice, optometry, and they do an exam — whatever they need to do to get a thorough history on you. The optometrist saw a lot of edema (swelling) in the back of my eyes, and it was bulging at the back of my optic nerves, so he referred me to the ophthalmologist. Ultimately, an MRI showed a brain tumor the size of an orange.
I had every symptom in the book. I had adapted to severe hearing loss that first appeared in high school before becoming completely deaf in my left ear by the time I was diagnosed. In basic training, I couldn’t balance and walk in a straight line. Everyone in my unit shunned me because they thought I wasn’t trying. We had to learn how to shoot a gun, and I could find the target in my vision, but then I couldn’t focus on it anymore. During my technical training, I started projectile vomiting every morning and lost my spatial awareness at the top of the stairs.
At this point, I was not sleeping half the time because my migraines were so bad, and no one believed me. So I had quit talking and quit telling providers about it. I was having nightmares that I felt like I was dying, essentially.
[Once I knew it was due to an acoustic neuroma,] I felt like there was a light at the end of the tunnel because I knew there was a diagnosis behind it. It was a relief to have someone take my complaints seriously.” — Kayla S.
“Growing up, I was very klutzy. I basically broke every bone in my body from falling, tripping, or even rolling out of bed. I was also exhausted all the time. In high school, I was drinking six espresso shots a day just to keep my eyes open in class. I had severe migraines and vertigo so bad that I almost got into a car accident once when I turned my head while driving.
At the time, I didn’t have an explanation for any of it. I just thought maybe I was clumsy, tired, or pushing through what everyone else pushed through. Looking back, I know my body was trying to tell me something. I had a massive tumor pressing against my brainstem, causing extreme fatigue and balance issues.
The worst symptom was my hearing, but I kept making excuses for that, too. I thought maybe it was from swimming or loud workout classes. Then, in April 2021, I was on a plane with my boyfriend and offered him my headphones. I told him, ‘The right ear is busted. It doesn’t work.’ He looked at me and said, ‘No, they work perfectly.’
We tested it by turning an AirPod all the way up in my ear, and I couldn’t hear a single thing.
That moment was terrifying, but it also changed everything. I went to an audiologist and found out my hearing was only at 3-5%. Because I was so young, they ordered my first MRI.
That MRI found a tumor that was four centimeters by four centimeters, pressing against my brainstem. My surgeon told me that if I had waited another week, it could have been fatal. I had to go into emergency 14-hour brain surgery.
I ended up losing all of the hearing in that ear as a side effect, but that surgery saved my life, kept the tumor contained, and saved my facial nerve. I don’t take that lightly. It was the beginning of a long road, but it was also the reason I’m still here.” — Nicky T.
“I had really bad vertigo, and I started to feel off. It started to feel reminiscent and similar to when I had a vertebral artery dissection a couple of years prior, so I went to my primary care provider because I was not feeling right. I would get dizzy and nauseous every time I was driving in my car, and I looked down to switch the fan, temperature, or radio.
With my history, she ordered an MRI for peace of mind that everything was OK. I found out I had two brain tumors — an acoustic neuroma and a meningioma. I was very shocked.
Given the pea-sized acoustic neuroma, they talked through my options and suggested the ‘watch and wait’ approach.” — Sarah D.
Treatment Options
Typically, patients have a few options after receiving an acoustic neuroma diagnosis: observation, surgery, or radiation therapy.
“I start my conversation with patients by framing what the treatment options are and the likely consequences,” Dr. Jackson said. “For the vast majority of patients, there is no one-size-fits-all. There are cases where one option upfront makes more sense for a particular person and outcome, but in the vast majority of cases, patients are presented with this menu of options to navigate.”
Observation
Vestibular schwannomas are typically slow-growing tumors, so for many patients, the “watch and wait” approach of regular MRI scans can be an option. If a later scan reveals the tumor is growing or symptoms are worsening, other treatment options can be discussed.
According to the MD Anderson Cancer Center, “the average tumor growth is estimated at one to two millimeters per year.” For comparison, the thickness of a standard credit card is about 1 millimeter, and two millimeters would look like the thickness of a U.S. nickel.
“In a lot of cases, treatment upfront is not the right move,” Dr. Jackson said. “We watch a lot of these tumors for a long time, and that’s part of trying to minimize the impact on your life. Some people choose to wait, knowing that the hearing eventually will probably go away with the tumor, but the surgery would do it faster, or radiation would do it faster. These are all parts of the conversations we have.”
While some acoustic neuromas can grow quickly, “about 33% of tumors don’t grow at all, and one to two percent get smaller without any treatment,” per Penn Medicine.
“I haven’t experienced hearing loss or tinnitus — just balance has been a big issue for me,” said Sarah D., who opted to watch and wait after her diagnosis. “If I can manage the symptoms I have right now, I would rather take the ‘watch and wait’ approach. There are some people who have these tumors, and they never grow, so it’s just symptom management. Vertigo has been terrible, but I’ve been able to manage that through physical therapy and some vestibular strengthening.”
Surgery
Surgery may be recommended for patients with large tumors, serious symptoms, hydrocephalus, or tumor growth. This operation aims to remove as much of the tumor as possible while preserving key functions, such as hearing (when possible) and smiling.
“Surgery is a cure for these tumors the vast majority of the time,” Dr. Jackson said. “With surgery, we can sometimes save the hearing that’s there for the right patient. If hearing is statistically likely to be preserved at surgery, it may make sense to do surgery earlier and in a more aggressive fashion to try to give the best chance of saving hearing. Or in some patients, if the tumor is big enough and the hearing is bad enough, the truth of the matter is that even if you saved the hearing they have, it’s not functional, so that’s not necessarily a big driver of surgery.”
These surgeries typically involve a neurosurgeon and a neurotologist, who is an ENT with specialized surgical training in treating hearing conditions, balance, and other ear disorders.
Surgical Approaches
Choosing a surgical approach is about finding the best pathway to get to the tumor. Surgeons pick the route based on a variety of factors, including the tumor’s size and location, the patient’s anatomy, surgical expertise, and whether they are able to save the patient’s hearing.
According to Johns Hopkins, “roughly half of patients with the smallest tumors who have useful hearing before surgery will maintain useful hearing after surgery.”
Acoustic neuroma surgery is considered microsurgery because the surgeon spends most of their time working through an operating microscope, which provides a high-definition view of the surgical area, while using specialized, ultra-fine instruments. Without the magnification of microsurgery, it would be nearly impossible to remove the tumor without damaging those hair-thin nerves.
In the middle cranial fossa approach, the surgeon makes an opening above the ear to reach the tumor from the top. This approach can be used for very small tumors and to preserve the patient’s hearing.
The retrosigmoid approach involves making an opening behind the ear, near the back of the head. This path allows the surgeon to see the tumor, the brainstem, and critical nerves — like the ones that control hearing and facial movement — all at once. It can be used for tumors of any size and may help preserve hearing.
In the translabyrinthine approach, the surgeon goes directly through the inner ear bone (the labyrinth), resulting in permanent hearing loss in that ear. The translabyrinthine approach may be used when the patient has already lost most or all of their hearing.
Radiation Therapy
Radiation therapy may be used:
To treat smaller vestibular schwannoma tumors
When other medical conditions or age prevent surgery
After surgery, if the entire tumor couldn’t be removed
Radiation treatment aims to stop the tumor from growing. While radiation doesn’t physically remove the tumor, the tumor may shrink over time.
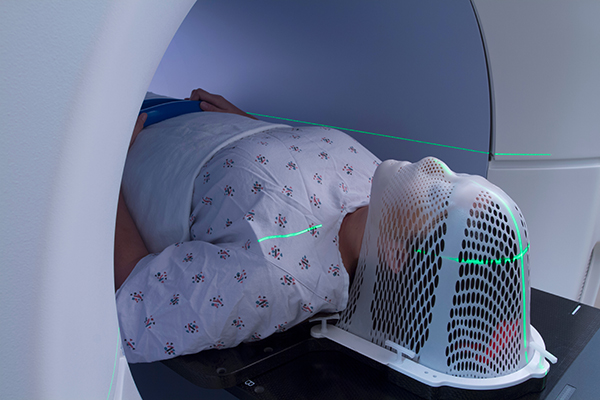
Some patients may undergo stereotactic radiosurgery (such as Gamma Knife). Despite the name, this treatment is not an actual surgery and requires no incisions. Instead, the treatment delivers targeted, high-dose radiation that acts like an invisible scalpel, pinpointing the tumor while sparing the surrounding healthy tissue. According to Mayo Clinic, this type of radiation therapy is “often used to treat small acoustic neuromas, usually less than 2.5 centimeters in size.”
Other patients may receive either traditional radiation therapy, which uses X-ray beams (photons) that pass through the tumor and continue beyond it, or proton therapy, which uses proton particles that release their energy directly at the tumor and then stop.
“Once I recovered from my second brain surgery, I did 26 sessions of photon beam radiation,” Jonathan said. “Toward the latter half of treatment, I always felt very tired, and my appetite was not really there. I also really struggled with nausea, but it gave me a lot of reassurance knowing the effectiveness of the radiation.”
Getting a Second Opinion
Receiving an acoustic neuroma diagnosis may feel overwhelming. Getting a second opinion about treatment options — observation, radiation, and surgery — is one of the most important steps a patient can take. National Brain Tumor Society, in partnership with the AANS/CNS Section on Tumors, encourages patients to seek a second opinion before brain surgery when it’s safe to do so.
“With the exception of giant tumors that are causing brainstem symptoms, there is time for second opinions,” Dr. Jackson said. “There is time to think through, talk with family members, and plan. Don’t let the weight of a brain tumor diagnosis rob you of that opportunity to really think through it and manage it. With a tumor that is relatively rare, I think there’s an enormous value in getting a second opinion, third opinion, or fourth opinion.”
Here are reasons why a second opinion is beneficial for acoustic neuroma treatment:
There is no one-size-fits-all approach. Every tumor and every patient is different. A second opinion helps lay out a menu of options, ensuring the treatment fits the patient’s unique tumor and goals.
Doctors have different philosophies. For example,not every doctor manages risk the same way. One surgeon may prioritize leaving a small piece behind to protect one’s nerves, whereas a second surgeon may remove the whole tumor at the expense of a nerve. A second opinion allows patients to find a care team that shares their values.
A second opinion gives the patient some control back. A patient can’t control that they have a diagnosis or the symptoms they’re facing, and they can’t control what a surgeon does once they’re under anesthesia or once the radiation beam is turned on. Dr. Jackson says, “But everything in between, you have choices, and so you should avail yourself of that.”
A second opinion can help increase confidence. If the second care team agrees with the initial assessment and treatment recommendation, patients can feel comfortable with their treatment decision.
Health systems can have different technologies available. A second opinion can introduce patients to the latest treatment options at other medical centers, potentially offering less invasive or more effective solutions.
“In the vast majority of cases, an acoustic neuroma is a manageable problem,” Dr. Jackson said. “Our goal is to have the tumor have the least impact on your life as possible, including the treatment of the disease itself and the psychological impact. It’s really important to partner with a treatment team you trust and feel is like-minded in helping you achieve that goal.”
Questions to Ask Your Potential Neurosurgeon
Acoustic neuromas are considered rare brain tumors, accounting for only 5% of all brain tumors, according to Dr. Jackson. High-volume surgeons have more experience working around the hair-thin cranial nerves to remove an acoustic neuroma. This level of expertise can make a difference when a tumor is in high-value real estate that can impact the ability to hear and smile.
“While there’s no hard and fast number, if somebody were to say [they do] less than 10 surgeries a year, I would probably wonder how much expertise they have in acoustic neuromas,” Dr. Jackson said. “The reality is in a lot of smaller centers — probably the vast majority of neurosurgeons and neurotologists — do less than 10 just because there’s just not that many [acoustic neuromas]. Doesn’t mean they couldn’t do a good job. It doesn’t mean that they’re not fantastic surgeons. It’s just that this surgery really does require a degree of expertise and a degree of familiarity being there every day.”
Consider asking any potential neurosurgeon the following questions to help make an informed decision.
How many acoustic neuromas do you operate on in a year? (Dr. Jackson recommends this question instead of ‘How many have you operated on in your career?’)
What percentage of acoustic neuromas do you radiate versus do surgery on?
What other specialists will be a part of my surgical team (e.g., anesthesiologist, neurotologist, etc.)?
Does your institution have a regular tumor board? If so, will my case be presented at that tumor board?
Are there clinical trials open for this type of tumor?
How might the recommended treatment/surgical approach impact my quality of life?
“I by no means am ever offended or concerned if somebody says they need to go get another opinion,” Dr. Jackson said. “Patients should never feel self-conscious or worried that the doctor will be offended.”
At the end of the day, patients need a treatment team they feel comfortable with.
Second Opinion Experiences & Tips
Community members generously shared their experiences getting a second opinion while considering their treatment options for vestibular schwannoma.
“The tough part was trying to decide, ‘Do you do radiation, or do you do surgery?’ It made for a challenging decision because each one has risks and benefits, and a different recovery timeline. I did a lot of research, and I talked to another physician who had an acoustic neuroma and had microsurgery. That was really helpful. I talked to a physician about radiation, too — just trying to get everybody’s perspective. I prayed about it and spent a lot of time talking with my wife about what would be the best next steps.
I’d encourage you to do your research, get a couple of opinions, and definitely see who you feel comfortable with. There are many great centers of excellence across the country, and people doing some really amazing work who perform these surgeries regularly and have experience with them. And the same thing with radiation, there are centers that treat a lot of these tumors. I would just encourage you to do the research and try to talk to other people who’ve had acoustic neuromas. It was helpful to hear their stories and experiences to feel like I’m not alone.” — Dr. Christopher S.
“So for me, with radiation versus surgery, I just really didn’t feel comfortable with the risks, because I was really at or over the line of tumor size to safely radiate. And so I just really didn’t like that option in my situation because of that. As far as the surgical approach, I had a larger tumor, and at that point, the likelihood of me retaining hearing was really, really low, because my tumor is already so large, and I had already lost most of that hearing.
I really found it was important for me, personally, to remove the hearing retention in my decision matrix. But the fact that I personally chose the surgical approach that would for sure make me deaf in that ear was really emotional. That was probably the most emotional day of the journey when I made that call. I sobbed to the doctor, as I told them over the phone.
The best advice that the original ENT, who told me I had a brain tumor, gave me was you have options. Look into them, meet with the doctors, talk to them, and then make the choice that you can live with and don’t look back. And that’s really what I did.
I’m 10 years out now from my surgery, and I still feel like I made a really good choice. The neurosurgeon said that my hearing nerve was totally on its last leg when they went in there. He was shocked I had any hearing at that moment. They were able to completely save my facial nerve, which is why the doctor really wanted to use the Translab approach, as he felt he would have a better view to preserve it.
If you get diagnosed with acoustic neuroma, it feels like it’s an emergency, and sometimes it is, if you have hydrocephalus or really emergent things going on, but most of the time, it’s not an emergency. It’s a slow-growing tumor, and it’s benign. You have the opportunity to do your research and pick your treatment.
I highly recommend that you do that and really look for places that see these regularly. It is considered a rare brain tumor, and outcomes really vary based on provider experience, so I would urge you to meet with lots of doctors, and don’t feel pressured into any one location, doctor, or even treatment type. I would explore your options, because that really does make a humongous difference in the outcomes, and it’s the rest of your life.
The variety of medical care really is huge. So often we’re trained to take whatever doctors say as gospel truth and just do what they tell us. And it can be really hard to buck that authority. It’s easy to just go with the first doctor. You should definitely shop around.” — Emily T.
“Ask everything. Do not leave a single question out if there’s a doubt in your mind about anything. Ask somebody and just alleviate all of that weight from your shoulders.” — Jonathan J.
“I went to a few different doctors in New York, and I got very different approaches and outcomes. One doctor said that I would likely not live very long and that I would not have a good outcome. The other doctor I saw said that I would be nearly deaf and that I would need to learn sign language.
When I went to NYU, they were very realistic. They said, ‘You could very possibly have facial paralysis. You very likely would be completely deaf on the left side.’ They were very straightforward. It wasn’t like they were hiding anything; it was just their outlook and their positivity that they’re going to do their best not to let those things happen. I was young, so they wanted me to live the rest of my life successfully. Their whole outlook and positivity just made me feel a lot more at ease than the other two doctors.” — Kat C.
“My biggest piece of advice is to seek more opinions. Don’t feel like you have to go with the first opinion you receive. Get two or three opinions, especially when you’re deciding on the next step in your care.
I didn’t do that at first. Later on, when I did get more opinions, doctors told me they would never have done the Gamma Knife. They would have operated on me.
That is hard to sit with, but it’s also why I share it. I want other people to know they are allowed to ask questions. They are allowed to slow down, get another perspective, and advocate for themselves.
I don’t think there is always one perfect answer. The right answer is the one you feel confident in — the one your heart can live with.” — Nicky T.
“I definitely listened to their opinions, knowing that they’re the experts and that they’ve seen this before, but then I also thought about what I want and what I want for the phase of life that I’m in right now.
I just wasn’t really ready to take that leap, especially because they gave me the hope that there are some people who have these, and they never grow, and they just manage symptoms. So I’ve always kind of had that hope in the back of my head of like, as long as I can manage the symptoms, I’m OK with taking that risk. If it ever comes to a point where my symptoms get so bad, or I eventually lose all my hearing. I might change my mind at that point and just be like, ‘Well, I lost my hearing. Let’s go ahead and take it out.’ But I’m not quite there yet to do it.” — Sarah D.
Benign is Not Fine
For many in the acoustic neuroma community, the word “benign” doesn’t feel like an accurate description of this diagnosis. It’s why the refrain “benign is not fine” gets used so much by survivors. As Allison L. puts it, “Benign sounds harmless, like it’s no big deal. But the truth is, it is a big deal. It didn’t mean what I was about to go through would be painless or easy.”
While these tumors aren’t cancerous, they can be life-changing.
Adapting to Hearing Loss
Emily T.
Many people with acoustic neuromas experience single-sided deafness (SSD), caused by either the tumor itself or the treatment to remove the tumor. Whether the hearing loss is gradual or sudden, adjusting to a new normal takes time — even realizing they need to sit where their hearing ear is facing others at a restaurant or crowded gathering.
“My first recommendation is to own your hearing loss — just tell people right off the bat — and feel comfortable in your own skin,” Nicky said. “The second tip is to not be intimidated or scared to get assistance, to get hearing aids, to put on those captions for accessibility, and just be comfortable with all the accessibility and assistance that you actually can have.”
“My first recommendation is to own your hearing loss,” Nicky said. “Tell people right off the bat, and try to feel comfortable in your own skin. I know that it is easier said than done, but hiding it only makes it harder. My second tip is not to be intimidated or scared to get assistance. Get the hearing aids. Turn on the captions. Use the accessibility tools available to you. For me, accepting help didn’t mean I was weaker. It meant I was giving myself what I needed to keep living my life fully. There is so much support out there, and you deserve to use it.”
Patients often turn to technology for accommodations and support.
Hearing Aids: Most patients with acoustic neuromas have a couple of hearing aid options. A contralateral routing of offside signals (CROS) hearing aid transmits sound from the non-hearing ear to the hearing ear. A bone-anchored hearing aid (BAHA) is a small implant that sends vibrations through the skull to the cochlea of the hearing ear. Some patients may have the option of a cochlear implant if their cochlear nerve remains intact and functional after treatment.
Over-the-Counter Hearing Solutions:AirPods Pro 2 and 3 have a Hearing Aid Feature (HAF), which the FDA approved as the first over-the-counter (OTC) hearing aid software device. HAF must be set up on an iOS device (an iPhone or an iPad). “For an over-the-counter solution, they have the absolute best background noise cancellation I have found,” Emily said. “Background noise is the nemesis of single-sided deafness. I love these AirPods for situations like a loud restaurant because it will cancel out the hubbub and really focus in on whoever you’re looking at. It’s a fabulous low-cost tool that can be really beneficial.”
Closed Captions: Turn on closed captions for the television, social media, Zoom meetings, and more to help the brain process what others are saying.
Smart Watch & Phones: Helpful apps can be paired with a smart watch or phone, allowing certain notifications to notify the person by vibration instead of sound.
“I use my smart watch to be my alarm because I don’t hear an alarm when I’m sleeping on my hearing ear,” Emily said. “I use a Ring doorbell so that my phone or smart watch vibrates when somebody comes to my house because I don’t hear the doorbell or someone knocking. There’s a lot of different technology that you can use to help your life.”
Managing Balance Difficulties
A person’s sense of balance is informed by their eyes, inner ears, proprioception (the physical feeling of touch), and their brain processing all of this input. An acoustic neuroma can disrupt one’s balance as it compresses the vestibulocochlear nerve, which sends signals from the inner ear to the brain about head position and movement for processing.
The brain, which is used to receiving signals from the vestibulocochlear nerve on both sides of the head, suddenly finds itself only getting clear information from one. This mismatch can lead to dizziness, unsteadiness, or even a disorienting sensation.
Vestibular rehabilitation can help train the brain how to process helpful signals from other places to compensate for the missing or incomplete information from the vestibulocochlear nerve on one side.
“When you first are doing vestibular rehabilitation after surgery, you can’t walk and move your head, because you’ll get off balance,” Emily said. “Moving around your head and moving around your eyes while walking, that’s too much. Your brain can’t figure out where you are. If you want to get back to regular life, you need to be able to do all of these layered things and walk. Vestibular rehab is teaching you the stepping stones to get back to it.”
These exercises typically focus on gaze stabilization (keeping vision stable during head movement), balance training, and habituation (desensitizing the brain to specific movements that cause dizziness).
“One of the best things I ever did was [go to] an amazing vestibular therapist,” Christopher said. “She gave me a lot of confidence. I was on a walker at that point, and she put me in a harness and had me start working on things. I went from the walker to hiking poles to walking without any help within a day or two.”
Addressing Facial Weakness & Paralysis
The facial nerve sits right next to the vestibulocochlear nerve, and this nerve is responsible for carrying signals involved in facial expression and movement. The facial nerve also plays a role in taste in part of the tongue and in producing tears. Given the close proximity, the facial nerve can be impacted by an acoustic neuroma or during treatment, which can result in temporary or permanent facial weakness or paralysis for some patients.
“Facial weakness is obviously always a big discussion within these cases,” Dr. Jackson said. “There are different rates that are reported. In the vast majority of cases, facial weakness can be avoided. Sometimes it’s the expense of leaving a little bit of tumor behind, particularly in bigger tumors. We’ve actually published on this quite a bit, even recently. Depending on what somebody’s baseline health is and how bad the facial weakness is, and when it comes on, will very much dictate whether or not that recovers. A lot of people will recover if there’s sort of temporary facial weakness, but there’s a risk that that will linger.”
Lived Experiences:
“I did wake up from surgery, and unfortunately, I did have facial nerve palsy. My nerve was intact. It just got stunned. Waking up to the fact that my face wasn’t working was very challenging, in addition to some of the challenges that went with that — trying to keep my eye moist and eating.
I remember being at church on Christmas seven days after my surgery and just hoping I could smile by Easter. I was getting frustrated because I felt like the facial nerve wasn’t going anywhere. We took pictures at Easter mass, and all of a sudden, I could see my upper teeth, and my smile was pretty close [to normal], which is amazing. It feels like things aren’t going anywhere, but it comes quickly.” — Christopher S.
“One whole side of my face is numb. It’s kind of like when you go to the dentist, and you get numb — you can kind of feel, but not that much. When I get tired, my eye droops, and my face will droop a little bit. I have really bad dry eye from it, too.
Going into brain surgery, facial paralysis was more of my concern than hearing because I had already had a hearing loss that I didn’t even know about. I was a teacher, and I taught second grade. With phonics, you need to be able to move your lips and whatnot.
Now, I use a straw when I drink anything. I get comments out all the time, ‘Why are you drinking wine with a straw?’ I just laugh at it now — I don’t really care. It didn’t impact me as much [as others] because I didn’t end up with a lot of facial paralysis.” — Kat C.
“Before my first surgery, they told me I might have temporary facial paralysis, and that they were going to do everything they could to protect my nerves. I did have temporary facial paralysis for about six months, but it slowly came back.
Unfortunately, after my next brain surgery, it didn’t come back. I’m someone who smiles at everything. I’m animated. I’m expressive. So when I couldn’t lift half of my face, I became really self-conscious.
Facial paralysis changes more than your appearance. It changes how you express joy, how you feel in photos, how you recognize yourself in the mirror, and how you move through the world. That part was really hard.
I wear sunglasses all the time. I even have night sunglasses. I have glasses for work. Part of that is because they help with my dry eye and the way my eye blinks, but they also make me feel more comfortable. And honestly, finding little things that make you feel more like yourself helps.
I also work really closely with my facial plastic surgeon, which I recommend for anyone dealing with facial paralysis. There are incredible doctors who specialize in Bell’s palsy and facial paralysis, and there are more options than people may realize. My surgeon would say things like, ‘We can do a little Botox here, a little lip filler here to even out your lips. We can add a small eyelid weight to help with blinking.’ There are solutions.
I’ve had to go through two major surgeries as part of this facial reanimation and reconstructive journey. It sounds really scary when you say it out loud, but it has actually been a really hopeful process because it is amazing what science can do.
Through a nerve graft and gracilis muscle transfer, my surgeon created what’s called a biting smile. Now, I can bite down to smile. It’s not a big, toothy smile, but after seven months of facial therapy, I had a smile again. I had to do smile exercises twice a day and train my body to bite whenever something was funny, so I could smile in the moment.
This past October, I had another surgery to hopefully create a spontaneous smile, so I won’t have to think about smiling anymore. It’s all about the long game. I have to wait about 11 months to see the full results, but I’ve already started to see improvement.
This journey has taught me that healing does not always mean going back to exactly who you were before. Sometimes it means learning your body all over again, accepting help, finding new ways to smile, and still choosing joy anyway.” — Nicky T.
Looking Ahead at Acoustic Neuromas
The future of identifying and treating acoustic neuromas is moving toward a molecular diagnosis, where Dr. Jackson believes we will eventually treat these tumors based on the tumor’s unique molecular and genetic features.
“I think we are at an inflection point where research is really going to push this to be a molecular diagnosis, where not every acoustic neuroma is going to be an acoustic neuroma, and we may even have biomarkers to know what it is before we even suggest a treatment,” Dr. Jackson said. “While that sounds a little bit like science fiction, that’s the way we treat tumors in almost every other scenario, other than these benign skull-based tumors. It’s an exciting time to be in this field both academically and surgically. I think there’s a lot of hope that this is something that we can push even further toward that goal of having minimum impact on people’s lives by a better understanding and better data.”
Patient & Caregiver Toolkit
Patients and caregivers are our top priority. National Brain Tumor Society equips patients and their care partners with the tools and resources they need to navigate every step of their unique health care journey — from understanding their diagnosis and building their medical team to making decisions about treatment, including accessing clinical trials and palliative care.
Explore our patient and caregiver toolkit to empower yourself with the resources and support you need throughout your brain tumor experience.