This website uses cookies that help the website function and that help us understand how you interact with it. Please read our privacy policy for more information.
“Immunotherapy” is one of the hot topics in cancer research right now. If you follow cancer and brain tumor research news, you have no doubt by now heard about this treatment approach recently. In fact, in both our recaps from the two biggest brain tumor-related scientific meetings in 2014 – American Society of Clinical Oncology (ASCO) and Society for Neuro-Oncology (SNO) – we noted how prevalent the topic was.
Dr. John Sampson, MD, PhD, MBA, MHSc
To help us and our community understand more about immunotherapies – what they are, how they works, promises, and challenges – we reached out to one of the leading experts in brain tumor immunotherapy, Dr. John Sampson from Duke University, who kindly dedicated his time.
Dr. Sampson is the Robert H. and Gloria Wilkins Professor of Neurosurgery, Chief, Division of Neurosurgery, and Associate Deputy Director of the Preston Robert Tisch Brain Tumor Center at Duke. Dr. Sampson is internationally recognized in the field and has received a number of national and international awards and grants in recognition of his expertise in neuro-oncology and especially in the area of immunotherapy for brain tumors.
This is the first of a two-part interview with Dr. Sampson. Some answers have been edited for length and clarity.
Q: What are “immunotherapies?” How do they work?
JS: The immune system is the part of the body that can recognize infections and destroy them. For cancer treatment, immunotherapy is the use of molecules from the immune system, or the activation of the immune system, to specifically recognize and destroy cancer cells while leaving healthy cells alone. Immunotherapies can be very specific for a protein produced by a tumor cell; this protein is the immunotherapeutic target.
Q: What is the promise of immunotherapies? How may they improve treatment outcomes compared to other treatments?
JS: Current treatments like chemotherapy and radiation are nonspecific and can only be given in doses that also causes harm to healthy tissue. Immunotherapy has the ability to be tumor-specific. Therefore, immunotherapeutic approaches have the potential to more effectively destroy tumor cells, while being less toxic to healthy tissue than current nonspecific treatments. Also, as immune cells have the ability to survey the body quickly and efficiently they can recognize tumor deposits away from the main tumor and may present a more effective means of treating cancer that has spread.
Q: What are the different types of immunotherapy?
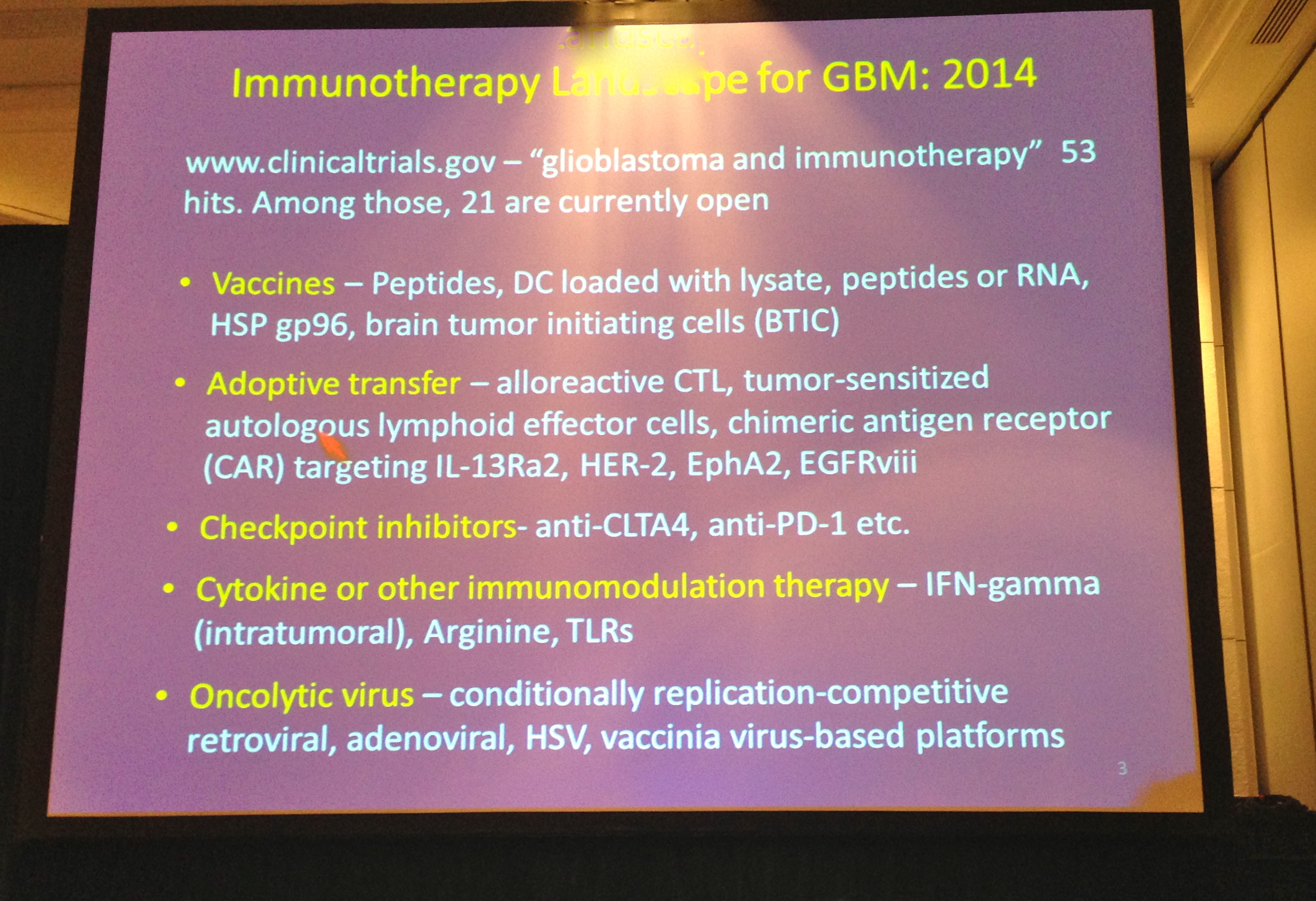
A: Immunotherapies can use: 1) molecules from the immune system, 2) cells from the immune system, 3) vaccination, 4) viruses, and 5) checkpoints to generate a therapeutic response (no particular order of importance).
In the first group, antibodies are molecules produced by the immune system that can specifically recognize a protein present on the surface of a cell and cause destruction of that cell. Tumor-targeted antibodies can be changed by researchers to carry toxic molecules directly to the tumor cell to induce tumor cell death. Immune-related molecules termed cytokines can also be given to patients to improve ongoing immune responses against tumor and are often used in conjunction with immunotherapy.
Types of immunotherapy discussed at the 2014 Society for Neuro-Oncology Annual Meeting
In the second category, cells of the immune system are also used in cancer immunotherapy. T cells are immune cells that can directly recognize and kill tumor cells if that tumor cell produces a molecule recognized by the T cell. Researchers can isolate tumor-specific T cells from patients, activate them outside of the body, and give them to the patient again in a process called adoptive transfer. T cells can also be genetically modified outside of the body before adoptive transfer in order to make them recognize a new tumor target.
With the vaccination approach, researcher use a therapeutic vaccine to begin an immune response against a tumor, much like how an immune response begins against a virus or bacteria. Two major types of immunotherapeutic vaccinations use dendritic cells (DCs) or tumor-specific protein. DCs are an immune cell that presents tumor-specific molecules to T cells to activate T cells recognizing those tumor targets and then kill tumor cells with those proteins. Tumor-specific protein given as a vaccine can be taken up by patient DCs within the body for the activation of anti-tumor immunity.
Oncolytic virotherapy is the fourth approach. In this case, a virus changed to selectively and safely recognize tumor cells is given to the patient to induce tumor-specific death.
Finally, an immune response can also be modified through the use of checkpoint blockades or checkpoint agonists. The body possesses several ways to change ongoing immune responses through “checkpoints” to ensure they do not become too strong (blockades to reduce ongoing immune responses) or too weak (agonists to enhance ongoing immune responses). An immune response to tumor can be strengthened through inhibiting a checkpoint blockade or through stimulating a checkpoint agonist.
Q: Have immunotherapies shown success in other cancers? If so, where has it worked to date?
Dr. Sampson at the 2013 National Brain Tumor Society Advancing Research to Treatments for Brain Tumors Meeting
JS: It is only recently that the potential of cancer immunotherapy has begun to be realized and there have been some astonishing successes. Among the most significant results come from the adoptive transfer of patient-derived anti-tumor T cells in the treatment of melanoma. This has shown objective response rates (tumor shrinkage) of 49-72% in patients with melanoma. Adoptive transfer of genetically modified T cells producing chimeric antigen receptors (CARs) has been most extensively tested in the context of leukemia and lymphoma. CARs introduce a new anti-tumor specificity to the T cells and T cells with CARs targeting a molecule called CD19 have shown an overall 80% response rate in acute lymphoblastic leukemia. Vaccination with tumor proteins has also shown promise. In melanoma, vaccination with a protein called gp100 and the cytokine interleukin-2 demonstrated improved progression free survival. In a small trial of women with the cancer vulvar intraepithelial neoplasia, 78% of women immunized with a mixture of thirteen tumor proteins demonstrated objective responses.
However, perhaps one of the biggest recent breakthroughs has been in the manipulation of immune checkpoint blockade. When an immune molecule called cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) is activated it weakens ongoing immune responses. An antibody specific for CTLA-4 (ipilimumab) blocks CTLA-4 function and allows the strong immune response to continue. In several large clinical trials the addition of ipilimumab by itself or in conjunction with standard therapy or immunotherapy shows significantly improved survival in treated patients. This suggests ipilimumab can strengthen anti-tumor immune responses already present in the patient and can improve immune responses from immunotherapy as well.
***
In Part II of this interview, Dr. Sampson discuss that specific applicability of immunotherapy for brain tumors, the challenges and progress made in using immunotherapies in the Central Nervous System, and some of the immunotherapy projects Duke is working on.
Your Brain Tumor Awareness Month gift has an immediate impact, supporting patients, driving advocacy, and funding groundbreaking research. Right now, thanks to a challenge from the Robert Lloyd Corkin Charitable Foundation, your gift is worth even more — help us raise $200,000 during the last six days of May to unlock an additional $30,000.