Fertility preservation may not be top of mind when a patient learns of their brain tumor diagnosis. Still, pediatric patients and patients of childbearing age may want to consider it before undergoing treatment.
Chemotherapy and even surgery and radiation, depending on the tumor’s location, can affect one’s fertility, which is why patients need to determine whether or not they would like to undergo fertility preservation before starting treatment.
Both the American Society of Clinical Oncology (ASCO) and the American Society of Reproductive Medicine (ASRM) recommend that every patient of reproductive age diagnosed with a malignancy that will require anti-cancer treatment should be seen by a reproductive specialist.
“Every single patient should hear from oncologists that this is the type of conversation they should have,” said Anna Sokalska, MD, PhD, the director of the Fertility Preservation Program at Stanford University School of Medicine. “It doesn’t mean that they have to go through fertility preservation, but at least they are fully informed what their options are and what potential obstacles are in the particular clinical case the patient is presenting.”
Learn more about how brain tumors and treatment can cause infertility, standard fertility preservation options, important questions to consider, and tips to manage the financial challenges that can come with fertility preservation.
The Impact of Brain Tumors on Fertility
A patient’s tumor location, as well as the type of medications and treatment they receive, can affect their fertility temporarily or permanently.
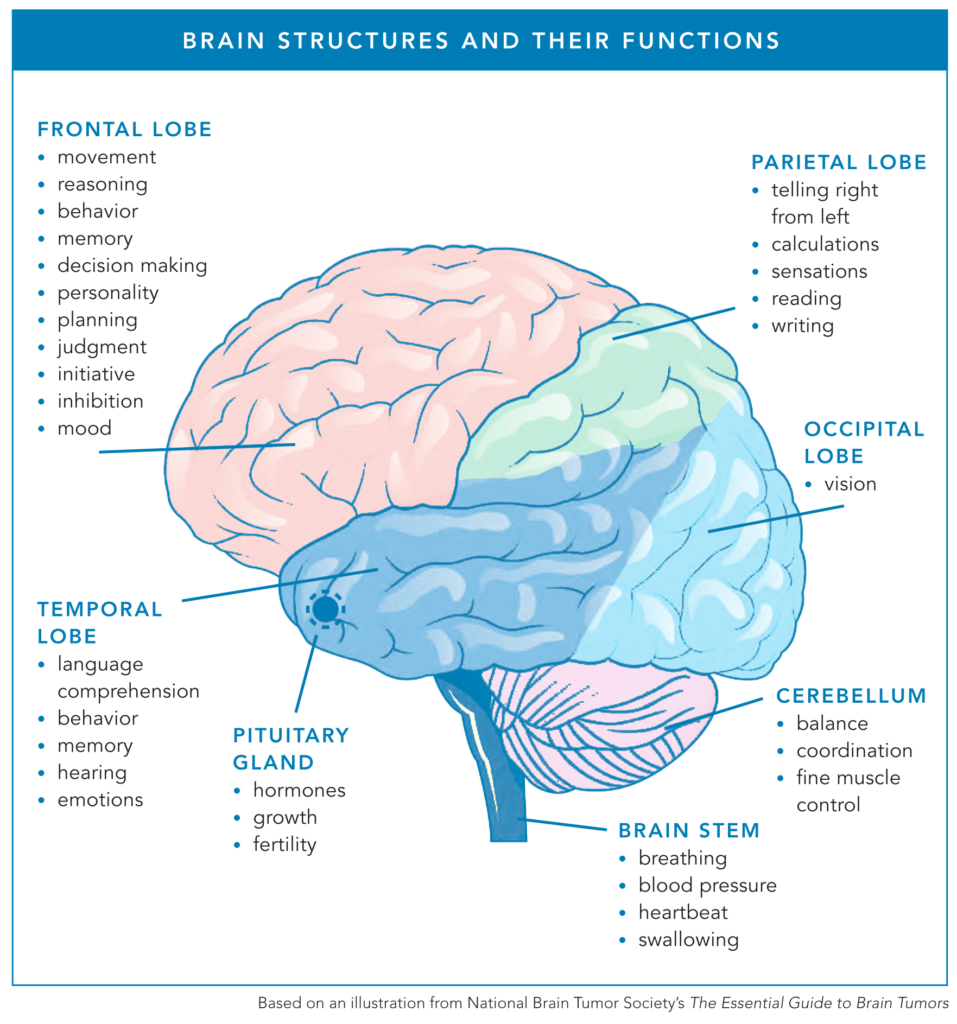
Pituitary Tumors
The pituitary gland is a small, pea-sized gland located at the base of the brain, and it interacts with the hypothalamus to coordinate various hormonal processes that impact fertility.
In men, the pituitary gland releases hormones that stimulate the testes to produce sperm and the male sex hormone, testosterone. For women, the pituitary gland plays a crucial role in regulating fertility by secreting hormones that control the menstrual cycle and support reproductive functions.
When a tumor encroaches on the pituitary gland, surgery and/or radiation may affect the function of the pituitary gland and, thus, one’s fertility.
“This type of infertility is kind of easy to fix [in women],” Dr. Sokalska said. “If the patient does not also get chemo, it’s not actually affecting the number of eggs. There is an easy way to overcome this problem by giving FSH and LH — the medication given for IVF stimulation. The patient can carry the pregnancy even if the pituitary function is affected.”
Clinical Trial Treatment
The impact of clinical trial drugs or devices on a patient’s infertility can be unknown. Fertility preservation ahead of a clinical trial may help provide peace of mind.
“Knowing that we were going into a trial where Julio was going to receive an experimental drug, we were concerned about fertility for the future because there was no knowledge of what this drug might do for fertility,” said Liz P., whose husband has ependymoma. “They didn’t know if and when it would ever be safe to conceive after receiving the medication, so we did take steps to pursue fertility preservation for Julio at that point.”
Tumor Treating Fields
Tumor Treating Fields (TTF), such as Optune, have not been evaluated to determine how they might impact one’s fertility. Additionally, they have not been tested on pregnant women to identify side effects or whether the treatment would be effective during pregnancy.
According to Novocure’s Instructions for Use for Optune, “Do not use Optune if you are pregnant, you think you might be pregnant, or are trying to get pregnant. If you are a woman who is able to get pregnant, you must use birth control when using the device.”
Chemotherapy
While other drugs used in cancer treatment may come with fertility risks, chemotherapy is known to affect fertility.
Women
Women are born with a finite number of eggs, ranging from half a million to two million eggs. By a woman’s first menstruation, her egg count is closer to 300,000-500,000 eggs. As women age, their egg count decreases without a way to produce new eggs.
Chemotherapy depletes a patient’s number of available eggs. The extent of the reduction depends on several factors, including a patient’s age (how many eggs they likely have prior to treatment), the duration and dose of chemotherapy, and the type of chemotherapy given to the patient.
Chemotherapy drugs classified as alkylating agents are the most dangerous to a patient’s egg count. Two chemotherapy drugs frequently used to treat brain tumors — temozolomide and lomustine — are both classified as alkylating agents.
Men
Chemotherapy can cause fertility issues, including damage to sperm, a lower sperm count, or even the inability to make semen. As with women, alkylating agents are the most damaging chemotherapy drugs when it comes to fertility.
“Because I wanted kids, especially through the diagnosis, I put some sperm away just in case,” said Michael S., who has anaplastic astrocytoma.
Timing of Fertility Preservation
Given that chemotherapy is the most significant fertility risk, undergoing fertility preservation would ideally be done prior to the start of chemo. When brain surgery is not urgent, the process could be completed before surgery.
Neuro-oncologists generally start patients on chemotherapy and radiation weeks after surgery, if surgery is needed. This gap between surgery and the start of chemo would allow time for female patients to freeze their eggs or embryos before treatment begins.
“No one will give a patient [ovarian] stimulation immediately after surgery because they need to recover,” said Dr. Solkaska. “You can get the preparation when [the patient is] recovering and actually proceed with the fertility preservation before starting the chemotherapy. It takes about 2-3 weeks to go through the entire fertility preservation process [freezing eggs or embryos].”
Unfortunately, not all health care providers will bring up fertility preservation after a brain tumor diagnosis.
“My wife is a CRNA, and I’m a nurse, but even with some medical background, we were unsure of where to start the process,” explained Megan C., who has oligodendroglioma. “Unfortunately, my care team didn’t ask us about fertility options until after my craniotomy and the week of starting radiation/chemo. Luckily, my wife had the insight to pursue it on our own. We got fast-tracked and had my eggs retrieved before starting treatment. I’m so grateful because we only had two embryos make it through. We miscarried one and had our rainbow baby in 2022.”
Questions to Ask Your Health Care Provider
Upon learning of a brain tumor diagnosis, there are questions one can ask their health care provider, such as a neuro-oncologist, about fertility preservation prior to surgery or treatment. Consider these questions from the patient’s perspective:
- Given the type of treatment recommended for me, what is my fertility risk?
- Do you anticipate this potential infertility being temporary or permanent?
- Is there an oncofertility specialist or reproductive endocrinologist I could speak to before I begin treatment?
- Knowing my tumor type and treatment plan, when is the optimal time to start fertility preservation?
- Will it be safe for me to carry a pregnancy in the future? How long would I need to wait after treatment ends to try to conceive? If not, is surrogacy legal in my state?
If a patient does not get a referral from their neuro-oncologist, they or their significant other can look up a nearby fertility clinic and schedule an appointment independently. Be sure to explain the urgency of the appointment due to a cancer diagnosis. Fertility clinics can usually get patients with cancer in within a few days.
Questions to Ask a Reproductive or Fertility Specialist
Once an appointment is scheduled with a fertility specialist, there are questions patients can ask to help decide whether or not to move forward. Consider these questions from the patient’s perspective:
- In my particular case, which fertility preservation option is the most feasible?
- Do I truly need to have fertility preservation, given the type of treatment I am going to have?
- How safe will ovarian stimulation be for me? If stimulation is after my brain surgery, what can I do to mitigate my blood clot risk? (Ovarian stimulation is related to the elevated level of estrogen, which brings a risk of blood clots.) Do I need any particular medication?
- What is my recovery time from ovarian stimulation and egg retrieval?
- What would be the costs associated with fertility preservation given my insurance (both the procedure to freeze and any ongoing storage costs)?
- Do I have enough time to proceed with fertility preservation? If moving forward delays my cancer treatment at all, will the delay affect the outcome of my treatment?
- If I decide to move forward with freezing my sperm, eggs, or embryos, what are my options should I decide I no longer need them?
“I am so grateful to have been presented with these [fertility preservation options] so early on,” said Erin S., whose husband was diagnosed with glioblastoma. “Many don’t think to explore fertility options, considering they were just given such a grim prognosis. It is always a good idea, in my opinion, to try to always think ahead and be hopeful for the future.”
Fertility Preservation Options for Patients of Child-bearing Age
There are a handful of fertility options for patients of child-bearing age before treatment begins.
In this process, called sperm freezing or sperm banking, sperm is collected through ejaculation and then frozen for future use. This option is non-invasive with a high success rate. For men who do not need emergency brain surgery, it may be possible to freeze their sperm prior to surgery. If not, sperm collection can be done between surgery and chemotherapy. Since there is no medication or preparation needed for this collection, a decision to move forward can be made one day, with the collection made the next day.
“From one ejaculation, [a patient] may have several frozen vials,” said Dr. Sokalska. “If it is not enough sperm or the parameters of the sperm aren’t great, then he can repeat it several times before starting the chemo.”
Freezing sperm gives male patients the greatest options in the future. For example, their sperm could be used for intrauterine insemination (IUI) or in vitro fertilization (IVF) at a later time.
“Once we spoke to a genetic counselor, we were directed rather quickly to have my husband provide his sample to be frozen as we needed to have this completed prior to starting treatment,” Erin said. “I am so glad we were informed because we were told later on when pursuing IVF that his current sperm was not viable for reproduction.”
In instances where the male patient is physically unable to ejaculate, there is a procedure called microsurgical epididymal sperm aspiration that can surgically yield enough sperm for multiple IVF cycles.
“My boyfriend and I attempted to freeze his sperm, but we really needed surgical support for medical reasons, and regrettably weren’t prioritized for the procedure before he needed to start treatment,” said Lauren D., whose partner was diagnosed with glioblastoma. “It was heart-wrenching, a secondary loss for the both of us — he wanted me to have it in case I ever decide to be a single mother on my own.”
If the male patient has a long-term female partner, it is helpful to consider the age of his partner because her egg count is finite to determine when to pursue IUI or IVF — even if it’s while the patient undergoes treatment.
“I would say keep all your options open, even if you end up not using them,” Amina* said. “As a female caregiver, I wish I had preserved my own eggs because you never know how your desires and goals change in the future, should your loved one not make it. So, to me, it is a matter of considering fertility preservation both for the patient and their partner.”
Egg freezing allows women to preserve their eggs before cancer treatment by undergoing a two-week regimen of hormone shots to develop eggs. Then, the mature eggs are removed from the ovaries during a procedure and frozen without being fertilized. The amount of eggs will vary, but younger women may have a dozen or more collected. When the patient is ready to try to get pregnant or try surrogacy through a gestational carrier, the eggs can be thawed and fertilized in a lab.
Oocyte cryopreservation requires ovarian stimulation before egg retrieval, which can take 9-12 days. From the end of stimulation to the moment of egg retrieval, it can take a couple of days. At most, it should take about two weeks from when the patient starts stimulation to the moment they undergo egg retrieval. Chemotherapy can be started the next day.
Egg freezing gives the patient greater flexibility, but egg quality is unknown until it is fertilized with sperm to form an embryo.
“At the moment when you are freezing eggs, there is a lot of unknown about what will happen later,” said Dr. Sokalska. “When you freeze the eggs, you cannot say anything about the quality. Eggs are also more fragile to the freezing and thawing process, surviving in about 84-85%. Embryos are surviving in about 95-97%, so that is a significant difference.”
With embryo cryopreservation, the patient undergoes the same process as she would to freeze her eggs. Once the eggs are retrieved, they are fertilized in the lab with sperm from their partner or a sperm donor. The resulting embryos are then frozen for future use. When the patient is ready to try to get pregnant or try surrogacy through a gestational carrier, there would be an additional procedure called an embryo transfer when the embryos are transferred into the woman’s uterus.
“If a patient is in a stable relationship, is married, and knows that they would like to build a family with that particular partner, then the option will be embryo freezing,” Dr. Sokalska said. “Preserving embryos is slightly better for the reason that you cannot truly say anything about the egg quality when you’re freezing the eggs. Egg quality is verified at the moment we combine the eggs with the sperm and create the embryos.”
The ovarian stimulation and egg retrieval process is the same for egg and embryo freezing. Patients choosing to freeze their embryos can begin chemotherapy the day after egg retrieval, as the remainder of the embryo freezing process happens in the lab without patient involvement.
Ovarian suppression through Lupron injections involves the use of a medication called leuprolide acetate, commonly known as Lupron. Lupron belongs to a class of drugs called gonadotropin-releasing hormone (GnRH) agonists. It temporarily suppresses ovarian function by altering the natural hormonal signals that regulate the menstrual cycle.
These injections essentially put a patient in biochemical menopause to protect their ovaries during chemo. This medication disrupts communication between the hypothalamus, pituitary gland, and ovary. It is only given to the patient while they get chemotherapy.
“The data of what is the degree of protection to the ovaries, [and] the efficacy of giving a patient this type of medication is very mixed,” Dr. Sokalska said. “We truly don’t know how much protection it is giving to the ovaries. We never recommend this method as a solitary method. What are ASCO and ASRM recommending? Use this option if we do not have time, if we cannot do anything else, or as an additional layer to already freezing eggs or embryos. There is no harm in doing it in addition to freezing the eggs or freezing the embryos.”
Following a comprehensive review of the scientific literature, the American Society of Clinical Oncology recommended in vitro maturation (IVM) of oocytes (eggs) as “an emerging fertility preservation method prior to cancer treatment” in its latest 2025 fertility preservation guideline update.
Unlike IVF, IVM retrieves immature oocytes from small follicles in the ovaries and then matures them in an IVF lab. Because IVF requires mature oocytes from large follicles, it requires high doses of hormonal stimulation. On the other hand, IVM requires no or minimal hormonal stimulation. Additionally, there is no trigger shot needed in IVM, unlike a traditional IVF cycle.
Once the immature oocytes are retrieved and matured in the lab, the remaining steps follow the traditional IVF approach: fertilizing the mature oocytes with sperm.
A 2025 article in Reproduction and Fertility reports that this evolving technology “offers a less invasive and cost-effective alternative to conventional controlled ovarian stimulation” and is a beneficial option for patients facing urgent fertility preservation. That being said, the same article states, “Although IVM holds great promise, it is not yet widely used because its success rates are not as high as those of conventional methods.”
The 2021 American Society for Reproductive Medicine’s IVM Committee Opinion notes that this method is not available for every patient and that it “should be offered by those with expertise gained by specific training, and should always be accompanied by appropriate counseling about expected results and informed consent. This technology is no longer considered experimental.”
Questions to Help Determine Egg or Embryo Freezing
Both egg and embryo freezing are considered the gold standards for fertility preservation, according to Dr. Sokalska. From a patient’s perspective, here are questions to ask to help make that decision:
- Are you in a committed, long-term relationship where you feel comfortable having embryos with this partner as your only potential fertility option after treatment?
- Would you like to have the flexibility to have a baby with another partner in the event of divorce/breakup or your partner’s death? (“I do understand that they are committed to each other [now], but life is writing different scenarios,” Dr. Sokalska explained. “One of the things I always discuss with the patient is that freezing the eggs will give you this reproductive freedom in the future.”)
- Do I need to have a better understanding of the future size of my family? (After genetic testing, patients will know how many normal embryos they have in storage. “The chance of the live birth per one euploid embryo transfer is about 50-60%,” said Dr. Sokalska. “The advantage of preserving embryos is that you have a better understanding of where you are in terms of potentially having children.”)
- Do I or my partner have any genetic mutations we are concerned about passing down to potential children? (Dr. Sokalska shared, “Another very important thing, especially for cancer patients, is that if they’re carrying genetic mutations, which are predisposing them for the development of cancer, we can also do the testing of the embryos for that particular mutation and then pick the embryos without the mutation for transfer to avoid transferring abnormal genes to their offspring.”)
Fertility Preservation Options for Post-pubertal Pediatric Patients
For adolescent patients who are post-pubertal but under the age of 18, a reproductive specialist would talk with both the parent(s)/guardian(s) and the patient, as well as a private conversation with the patient.
“[The patient] still can say, ‘No, I don’t want to do it,’” said Dr. Sokalska. “It doesn’t matter what the patient’s parents want. This [choice] is ultimately the decision of the teenager. From my experience, a majority of the patients want to do something.”
Their fertility preservation options are the same as adults of child-bearing age.
“Our son was a teenager at the time of diagnosis,” Lisa* said. “For us, fertility preservation was an important decision and a highly emotional one, as it represented a leap of faith that he would survive into adulthood. Our son has told us that it means a great deal to him that we pursued this option.”
Fertility Preservation Options for Pre-pubertal Pediatric Patients
Pre-pubertal patients may not have developed mature eggs or sperm, but their gonads (ovaries or testes) are still susceptible to damage from cancer therapies. Preserving fertility empowers pediatric patients, as they grow older, to make decisions about family planning based on their own desires and circumstances. It allows them to have a say in their reproductive future rather than having limited options due to cancer treatments.
Recent advancements in fertility preservation techniques have expanded options for pre-pubertal patients, including ovarian tissue cryopreservation for girls and testicular tissue cryopreservation for boys.
Ovarian tissue cryopreservation is a fertility preservation technique that involves removing and freezing a portion of the ovary containing immature eggs (oocytes) for potential future use. This method is particularly relevant for pre-pubertal girls who have not yet reached reproductive maturity and, therefore, cannot undergo traditional methods of fertility preservation such as egg or embryo freezing.
Ovarian tissue cryopreservation is a newer option, as it was considered experimental until December 2019. Dr. Sokalska shares that there have only been about 200 live births from this method worldwide to date.
This option requires the patient to undergo at least two surgeries, which are typically laparoscopic procedures. In the first surgery, they remove one ovary or half of each ovary in order to freeze the cortex of the ovary, which is the superficial layer of the ovary where all the eggs are stored. The fertility clinic would then freeze the tiny pieces of that ovarian cortex, which is about 5mm x 1cm and has a thickness of 1mm. Later, when the patient is ready for pregnancy, the second surgery puts the tiny pieces of their ovarian cortex back.
“When we put these pieces of ovarian tissue back, there is a certain time required until the new blood vessels will grow into that ovarian cortex,” Dr. Sokalska said. “It can take several months until the function of this ovarian cortex is resumed. During this adaptation period, there is a reperfusion injury leading to the loss of almost 70-74% of the eggs in that ovarian cortex.”
Older patients who have a lower egg count will lose up to 74% of their eggs in that ovarian cortex, so this method may not result in pregnancy for them. Because of this, ovarian tissue cryopreservation is best suited for pre-pubertal girls or women unable to undergo ovarian stimulation for egg retrieval (e.g., the patient must start chemo in 2-3 days).
The transplantable ovarian tissue may only work for a few months or a few years after the second surgery, so the follow-up procedure should not be done until the patient determines they are ready to build a family and try to get pregnant.
Testicular tissue cryopreservation is a fertility preservation technique designed for pre-pubertal boys facing cancer treatment who are not yet able to produce sperm. This procedure involves the surgical removal of a small piece of testicular tissue, which contains immature sperm cells. The collected tissue is then frozen and stored for potential future use when the patient reaches reproductive maturity.
“Sadly, preserving a nine-year-old boy’s fertility was not brought up to us by any member of his extensive oncology team,” said Joy I., whose son had medulloblastoma. “A national fertility preservation team scheduled a testicle tissue sample surgery at the same time he was getting his port placed.”
Testicular tissue cryopreservation is still considered experimental, and no live births have resulted from using this frozen tissue. However, keep in mind that advancements in reproductive medicine may lead to changes in the status of this technique over time. According to The Oncofertility Consortium, “Anticipating that new therapies will be available in the future, many centers in the U.S. and abroad have determined that it is reasonable to preserve testicular tissue for young patients who are at high risk for infertility and have no other options to preserve their fertility.”
Questions to Ask While Considering Fertility Preservation
Undergoing fertility preservation comes with its own challenges. From a patient’s perspective, here are questions to help with one’s decision-making process:
- If I decide to move forward with fertility preservation, what would be my motivating factor?
- How does this decision align with my overall treatment goals and priorities?
- Which fertility preservation option makes the most sense, given my circumstances and goals?
- Is there any chance I may want to have a child biologically related to me one day?
- Are there alternative family-building options that I’m open to exploring (e.g., adoption or using donor sperm, eggs, or embryos)?
- Can I afford to undergo my desired fertility preservation method? Can I afford the annual cost to store my sperm, eggs, or embryos?
- Do I have any religious or ethical concerns about fertility preservation?
- Am I comfortable discarding my sperm, eggs, or embryos should I decide that I no longer want or need them?
- What would I want done with my sperm, eggs, or embryos if I were to pass away before they were used?
- If I have a partner, how do they feel about these questions?
“You really need to have an open discussion with your partner and make sure that this is the best decision for you,” said Payton F., who has oligodendroglioma. “I believe that the biggest decision throughout this process is whether or not to freeze eggs vs embryos. These are huge life-changing decisions that will potentially bring children into your life forever. This decision is very emotional to make.”
Revisiting Fertility After Cancer Treatment
If a patient does not have a chance to undergo fertility preservation before treatment, a reproductive specialist can evaluate their sperm count and quality or ovarian reserve after treatment.
“It doesn’t mean every single patient will be infertile after the treatment,” Dr. Sokalska explained. “Their number of eggs may be decreased. Their fertility window may be a little bit more narrow because they had the chemotherapy, but they may still be fertile. If we truly can’t do anything before treatment, we can recheck their ovarian reserve after the chemotherapy and potentially think about the egg freezing or embryo freezing for the time when they are ready to get pregnant.”
* Note: NBTS altered some patient or caregiver names to protect the privacy of the quoted individual.
Fertility preservation is a common quality of life concern for patients with brain tumors and their loved ones. The content in this blog post is for informational and educational purposes only. It does not constitute medical advice, nor is it a political statement. States may have different laws or restrictions regarding infertility treatment technology, as this is a shifting landscape, so please speak with your health care team to discuss your particular circumstances before making decisions.
Last Updated: February 10, 2026